Blood and Marrow Transplantation and Cellular Therapy, New York University Langone Health, New York, NY.
Division of Hematology, University of Torino, Torino, Italy.
Blood Adv. 2023 Jul 25;7(14):3604-3611. doi: 10.1182/bloodadvances.2023010545.
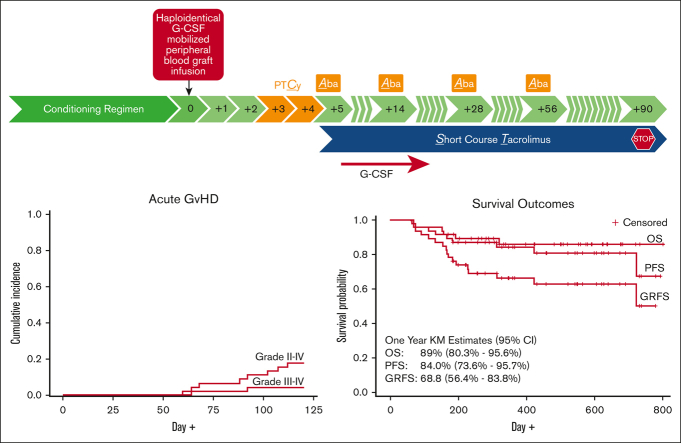
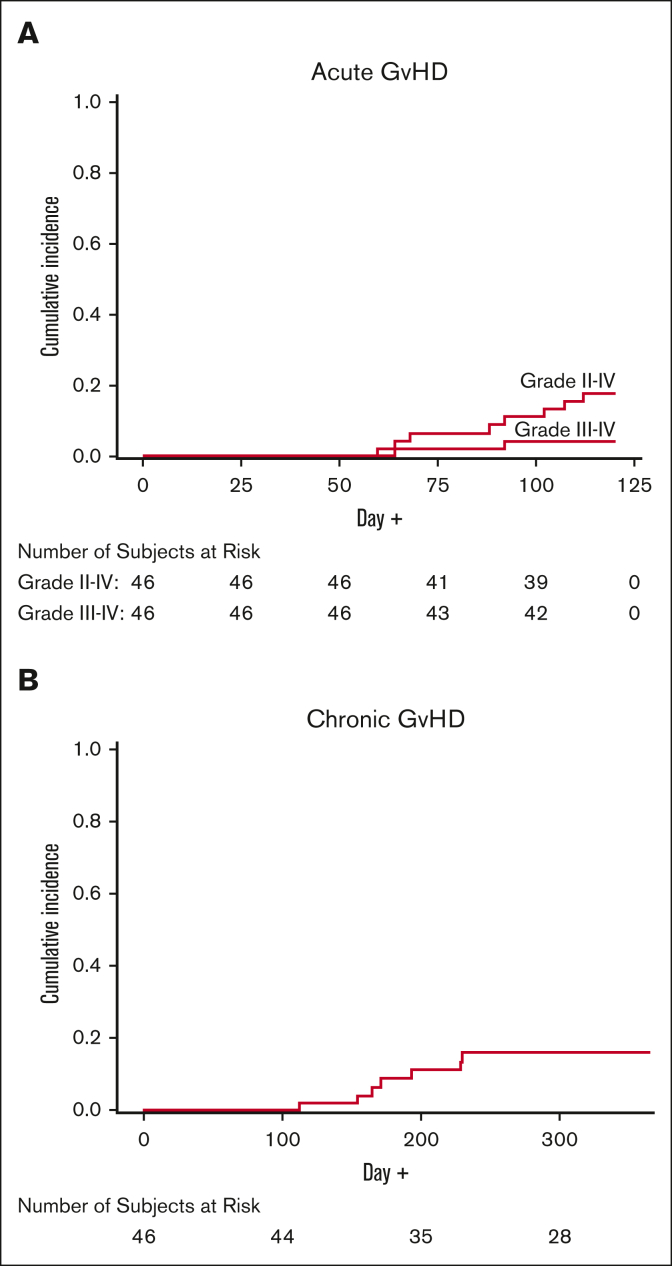
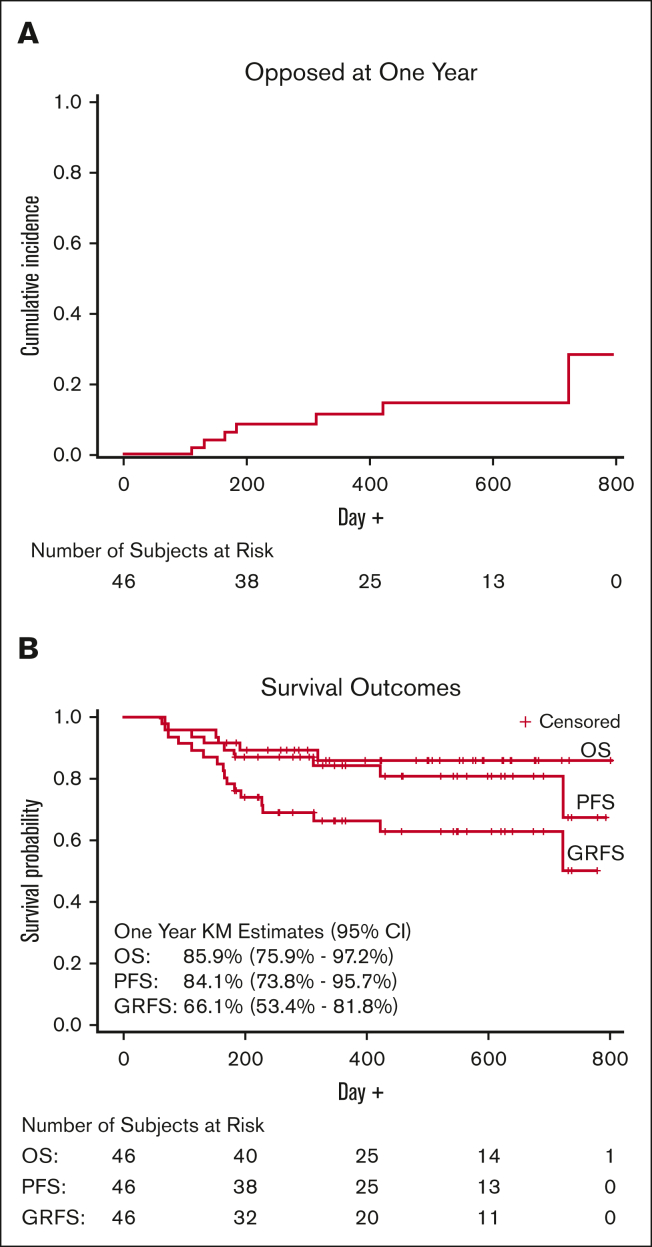
Reducing the incidence of graft-versus-host disease (GVHD) after haploidentical hematopoietic stem cell transplantation (HSCT) is warranted. Posttransplant cyclophosphamide (PTCy) is the main agent used for GVHD prevention in this setting. It remains unknown whether costimulation blockade can be safely combined with PTCy and enhance its efficacy. We performed a phase 1b-2 clinical trial to examine the combination of PTCy, abatacept, and a short course of tacrolimus (CAST) after peripheral blood haploidentical HSCT. The primary end point was the incidence of grades 2-4 acute GVHD by day +120. The study enrolled 46 patients with a median age of 60 years (range, 18-74 years). The cumulative incidences of grades 2-4 and 3 or 4 acute GVHD were 17.4% (95% confidence interval [CI], 9.2-32.9) and 4.4% (95% CI, 1.1-17.1), respectively. With a median follow-up of 15.3 months, the cumulative incidence of 1-year treatment-related mortality was 4.4% (95% CI, 1.1-17.1). The estimated 1-year moderate-to-severe chronic GVHD rate, relapse rate, progression-free survival, overall survival, and GVHD- and relapse-free survival were 15.9% (95% CI, 8-31.7), 11.7% (95% CI, 5-27.2), 84.1% (95% CI, 73.8-95.7), 85.9% (95% CI, 75.9-97.2), and 66.1% (95% CI, 53.4-81.8), respectively. Toxicities were similar to those expected in patients receiving haploidentical HSCT. This clinical trial showed that the CAST regimen is safe and effective in reducing the rate of grades 2-4 acute GVHD after haploidentical peripheral blood HSCT. This trial was registered at www.clinicaltrials.gov as #NCT04503616.
降低单倍体造血干细胞移植(HSCT)后移植物抗宿主病(GVHD)的发生率是有必要的。在这种情况下,环磷酰胺(PTCy)是预防 GVHD 的主要药物。尚不清楚是否可以安全地将共刺激阻断与 PTCy 联合使用并增强其疗效。我们进行了一项 1b-2 期临床试验,以研究外周血单倍体 HSCT 后 PTCy、阿巴西普和短程他克莫司(CAST)联合应用的情况。主要终点是+120 天的 2-4 级急性 GVHD 的发生率。该研究纳入了 46 名中位年龄为 60 岁(范围为 18-74 岁)的患者。2-4 级和 3 或 4 级急性 GVHD 的累积发生率分别为 17.4%(95%CI,9.2-32.9)和 4.4%(95%CI,1.1-17.1)。中位随访 15.3 个月后,1 年治疗相关死亡率的累积发生率为 4.4%(95%CI,1.1-17.1)。估计 1 年中重度慢性 GVHD 发生率、复发率、无进展生存率、总生存率、GVHD 和复发无生存率分别为 15.9%(95%CI,8-31.7)、11.7%(95%CI,5-27.2)、84.1%(95%CI,73.8-95.7)、85.9%(95%CI,75.9-97.2)和 66.1%(95%CI,53.4-81.8)。毒性与接受单倍体 HSCT 的患者预期的毒性相似。该临床试验表明,CAST 方案在外周血单倍体 HSCT 后降低 2-4 级急性 GVHD 的发生率方面是安全且有效的。该试验在 www.clinicaltrials.gov 上注册,编号为 NCT04503616。