Department of Surgery, Radboud Institute for Health Sciences, Radboud University Medical Centre, Nijmegen, The Netherlands.
Department of Surgery, Maastricht University Medical Centre+, Maastricht, The Netherlands.
Br J Surg. 2023 Jun 12;110(7):852-863. doi: 10.1093/bjs/znad123.
Anastomotic leak is a severe complication after oesophagectomy. Anastomotic leak has diverse clinical manifestations and the optimal treatment strategy is unknown. The aim of this study was to assess the efficacy of treatment strategies for different manifestations of anastomotic leak after oesophagectomy.
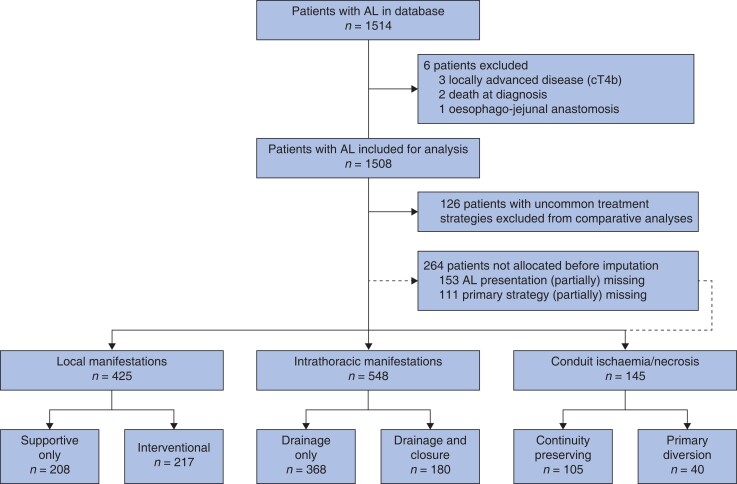
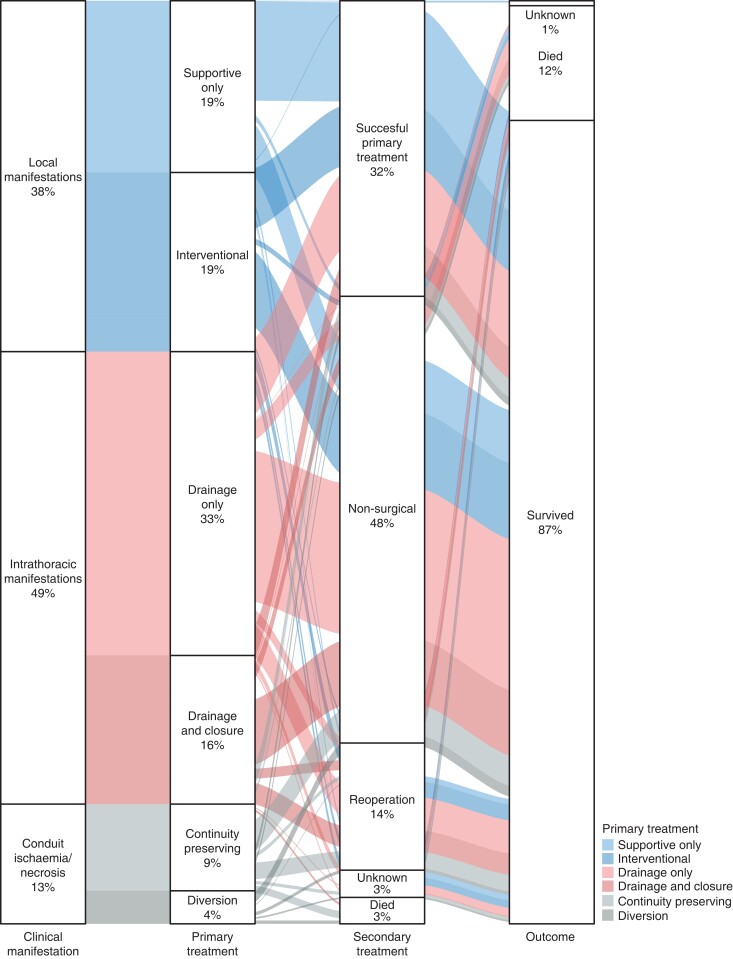
A retrospective cohort study was performed in 71 centres worldwide and included patients with anastomotic leak after oesophagectomy (2011-2019). Different primary treatment strategies were compared for three different anastomotic leak manifestations: interventional versus supportive-only treatment for local manifestations (that is no intrathoracic collections; well perfused conduit); drainage and defect closure versus drainage only for intrathoracic manifestations; and oesophageal diversion versus continuity-preserving treatment for conduit ischaemia/necrosis. The primary outcome was 90-day mortality. Propensity score matching was performed to adjust for confounders.
Of 1508 patients with anastomotic leak, 28.2 per cent (425 patients) had local manifestations, 36.3 per cent (548 patients) had intrathoracic manifestations, 9.6 per cent (145 patients) had conduit ischaemia/necrosis, 17.5 per cent (264 patients) were allocated after multiple imputation, and 8.4 per cent (126 patients) were excluded. After propensity score matching, no statistically significant differences in 90-day mortality were found regarding interventional versus supportive-only treatment for local manifestations (risk difference 3.2 per cent, 95 per cent c.i. -1.8 to 8.2 per cent), drainage and defect closure versus drainage only for intrathoracic manifestations (risk difference 5.8 per cent, 95 per cent c.i. -1.2 to 12.8 per cent), and oesophageal diversion versus continuity-preserving treatment for conduit ischaemia/necrosis (risk difference 0.1 per cent, 95 per cent c.i. -21.4 to 1.6 per cent). In general, less morbidity was found after less extensive primary treatment strategies.
Less extensive primary treatment of anastomotic leak was associated with less morbidity. A less extensive primary treatment approach may potentially be considered for anastomotic leak. Future studies are needed to confirm current findings and guide optimal treatment of anastomotic leak after oesophagectomy.
吻合口漏是食管切除术后的一种严重并发症。吻合口漏的临床表现多种多样,最佳治疗策略尚不清楚。本研究旨在评估不同治疗策略对食管切除术后不同吻合口漏表现的疗效。
本研究为全球 71 个中心的回顾性队列研究,纳入了食管切除术后吻合口漏患者(2011-2019 年)。对于三种不同的吻合口漏表现,比较了不同的主要治疗策略:局部表现(无胸腔积气;血运良好的吻合口)的介入治疗与单纯支持治疗;胸腔内表现的引流和缺损闭合与单纯引流;以及吻合口缺血/坏死的食管转流与连续性保留治疗。主要结局为 90 天死亡率。采用倾向评分匹配来调整混杂因素。
在 1508 例吻合口漏患者中,28.2%(425 例)有局部表现,36.3%(548 例)有胸腔内表现,9.6%(145 例)有吻合口缺血/坏死,17.5%(264 例)经多次插补后进行了分配,8.4%(126 例)被排除。经倾向评分匹配后,对于局部表现的介入治疗与单纯支持治疗(风险差 3.2%,95%置信区间-1.8%至 8.2%)、胸腔内表现的引流和缺损闭合与单纯引流(风险差 5.8%,95%置信区间-1.2%至 12.8%)以及吻合口缺血/坏死的食管转流与连续性保留治疗(风险差 0.1%,95%置信区间-21.4%至 1.6%),90 天死亡率无统计学差异。一般来说,采用范围较小的主要治疗策略后,发病率较低。
对于吻合口漏,采用范围较小的主要治疗策略与较低的发病率相关。吻合口漏的主要治疗方法可能需要进一步研究,以确认目前的研究结果,并指导食管切除术后吻合口漏的最佳治疗。