Saint Luke's Mid America Heart Institute, Kansas City, MO (M.E.N., S.L.W., K.G., B.A.A., T.K., M.N.K.).
University of Missouri-Kansas City (M.E.N., B.A.A., T.K., M.N.K.).
Circ Heart Fail. 2023 Jul;16(7):e009837. doi: 10.1161/CIRCHEARTFAILURE.122.009837. Epub 2023 May 19.
Patients with heart failure (HF) have a high burden of symptoms and physical limitations, regardless of ejection fraction (EF). Whether the benefits of SGLT2 (sodium-glucose cotransporter-2) inhibitors on these outcomes vary across the full range of EF remains unclear.
Patient-level data were pooled from the DEFINE-HF trial (Dapagliflozin Effects on Biomarkers, Symptoms, and Functional Status in Patients With Heart Failure With Reduced Ejection Fraction) of 263 participants with reduced EF (≤40%), and PRESERVED-HF trial (Effects of Dapagliflozin on Biomarkers, Symptoms and Functional Status in Patients With Preserved Ejection Fraction Heart Failure) of 324 participants with preserved EF (≥45%). Both were randomized, double-blind 12-week trials of dapagliflozin versus placebo, recruiting participants with New York Heart Association class II or higher and elevated natriuretic peptides. The effect of dapagliflozin on the change in the Kansas City Cardiomyopathy Questionnaire (KCCQ) Clinical Summary Score (CSS) at 12 weeks was tested with ANCOVA adjusted for sex, baseline KCCQ, EF, atrial fibrillation, estimated glomerular filtration rate, and type 2 diabetes. Interaction of dapagliflozin effects on KCCQ-CSS by EF was assessed using EF both categorically and continuously with restricted cubic spline. Responder analyses, examining proportions of patients with deterioration, and clinically meaningful improvements in KCCQ-CSS were conducted using logistic regression.
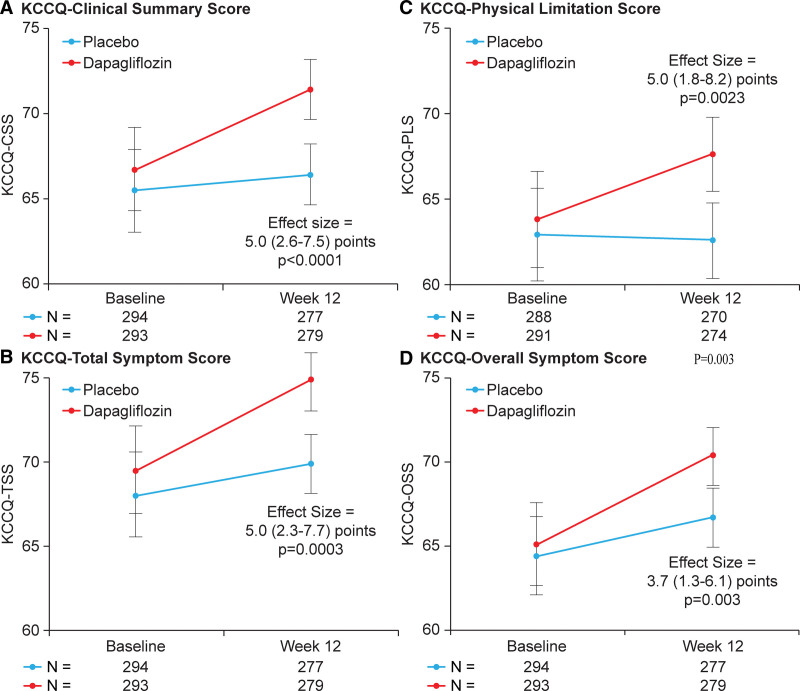
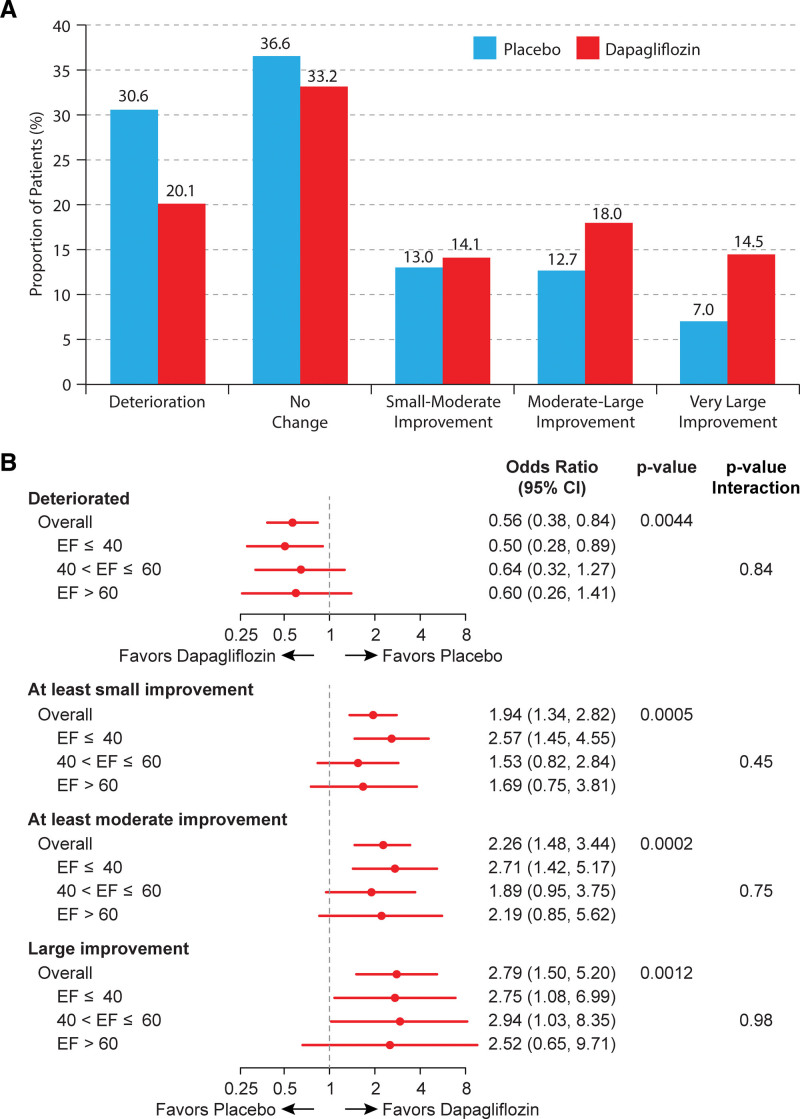
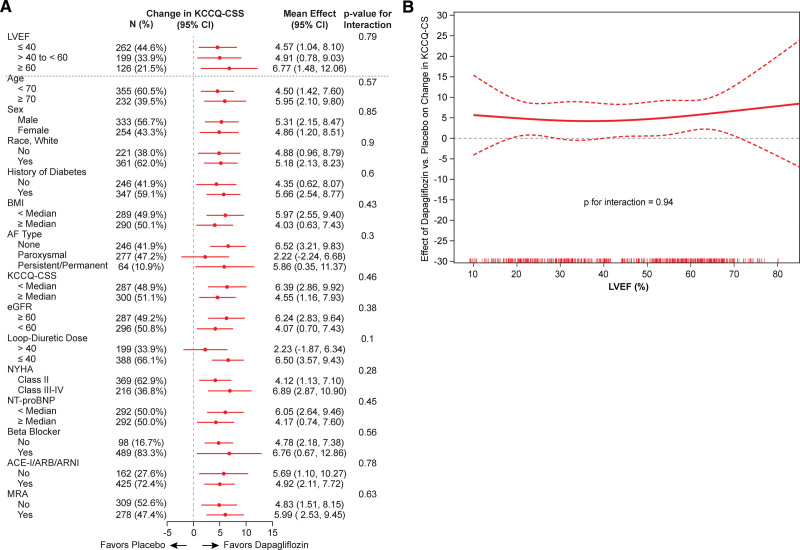
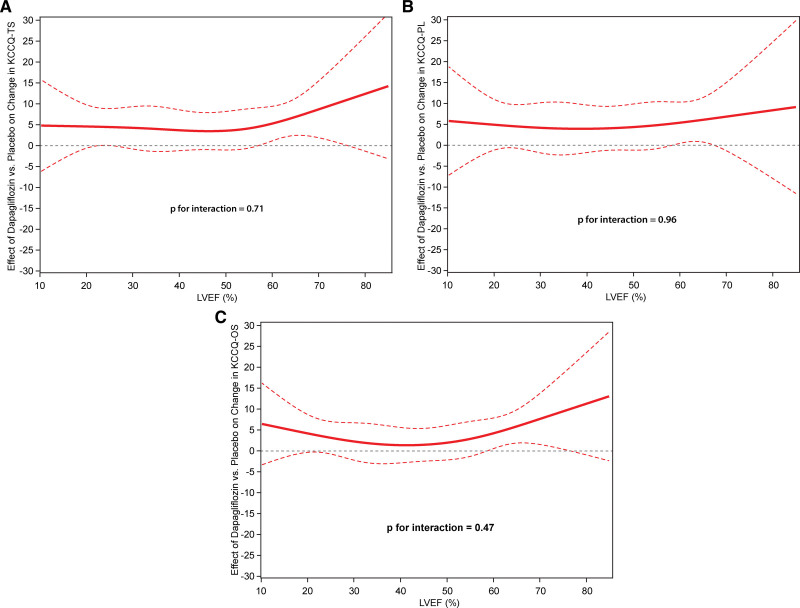
Of 587 patients randomized (293 dapagliflozin, 294 placebo), EF was ≤40, >40-≤60, and >60% in 262 (45%), 199 (34%), and 126 (21%), respectively. Dapagliflozin improved KCCQ-CSS at 12 weeks (placebo-adjusted difference 5.0 points [95% CI, 2.6-7.5]; <0.001). This was consistent in participants with EF≤40 (4.6 points [95% CI, 1.0-8.1]; =0.01), >40 to ≤60 (4.9 points [95% CI, 0.8-9.0]; =0.02) and >60% (6.8 points [95% CI, 1.5-12.1]; =0.01; =0.79). Benefits of dapagliflozin on KCCQ-CSS were also consistent when analyzing EF continuously (=0.94). In responder analyses, fewer dapagliflozin-treated patients had deterioration and more had small, moderate, and large KCCQ-CSS improvements versus placebo; these results were also consistent regardless of EF (all values nonsignificant).
In patients with HF, dapagliflozin significantly improves symptoms and physical limitations after 12 weeks of treatment, with consistent and clinically meaningful benefits across the full range of EF.
URL: https://www.
gov; Unique identifiers: NCT02653482 and NCT03030235.
心力衰竭(HF)患者无论射血分数(EF)如何,都有很高的症状和身体受限负担。SGLT2(钠-葡萄糖共转运蛋白 2)抑制剂对这些结局的益处是否因 EF 全范围而异尚不清楚。
从 DEFINE-HF 试验(Dapagliflozin 对射血分数降低的心力衰竭患者生物标志物、症状和功能状态的影响)和 PRESERVED-HF 试验(Dapagliflozin 对射血分数保留的心力衰竭患者生物标志物、症状和功能状态的影响)中汇总了 263 名射血分数降低(≤40%)和 324 名射血分数保留(≥45%)患者的患者水平数据。这两项试验均为随机、双盲、12 周的达格列净与安慰剂对照试验,招募了纽约心脏协会(NYHA)心功能 II 级或更高和升高的利钠肽的患者。采用协方差分析(ANCOVA)调整性别、基线 KCCQ、EF、心房颤动、估计肾小球滤过率和 2 型糖尿病,检验达格列净对 12 周时堪萨斯城心肌病问卷(KCCQ)临床总结评分(CSS)变化的影响。采用 EF 分类和连续受限立方样条评估达格列净对 KCCQ-CSS 影响的交互作用。使用逻辑回归进行患者恶化和 KCCQ-CSS 临床显著改善比例的应答分析。
在 587 名随机患者中(达格列净 293 名,安慰剂 294 名),EF 分别为≤40%、>40%≤60%和>60%的患者分别为 262 名(45%)、199 名(34%)和 126 名(21%)。达格列净在 12 周时改善了 KCCQ-CSS(安慰剂调整差异为 5.0 分[95%CI,2.67.5];<0.001)。在 EF≤40 的患者中(4.6 分[95%CI,1.08.1];=0.01)、>40≤60 的患者中(4.9 分[95%CI,0.89.0];=0.02)和>60%的患者中(6.8 分[95%CI,1.512.1];=0.01;=0.79)均一致。当连续分析 EF 时(=0.94),达格列净对 KCCQ-CSS 的益处也一致。在应答分析中,与安慰剂相比,接受达格列净治疗的患者恶化的比例更少,而 KCCQ-CSS 改善的比例更小、中度和大,这些结果在 EF 方面也一致(所有值均无统计学意义)。
在心力衰竭患者中,达格列净在治疗 12 周后显著改善了症状和身体受限,EF 全范围内具有一致且具有临床意义的益处。
NCT02653482 和 NCT03030235。