Papiris Spyros A, Kolilekas Lykourgos, Rivera Natalia, Spanos Michail, Li Guoping, Gokulnath Priyanka, Chatterjee Emeli, Georgakopoulos Alexandros, Kallieri Maria, Papaioannou Andriana I, Raptakis Thomas, Apollonatou Vasiliki, Antonogiannaki Elvira-Markela, Gialafos Elias, Chatziioannou Sofia, Grunewald Johan, Manali Effrosyni D
2nd Pulmonary Medicine Department, Medical School, General University Hospital Attikon, National and Kapodistrian University of Athens, Athens, Greece.
7th Pulmonary Department, Athens Chest Hospital "Sotiria", Athens, Greece.
Front Med (Lausanne). 2023 May 10;10:1174518. doi: 10.3389/fmed.2023.1174518. eCollection 2023.
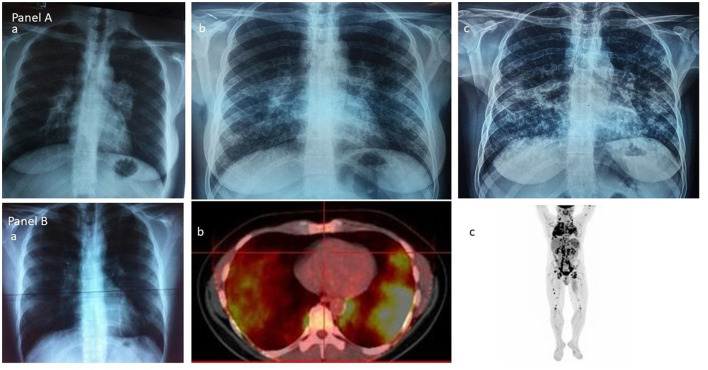
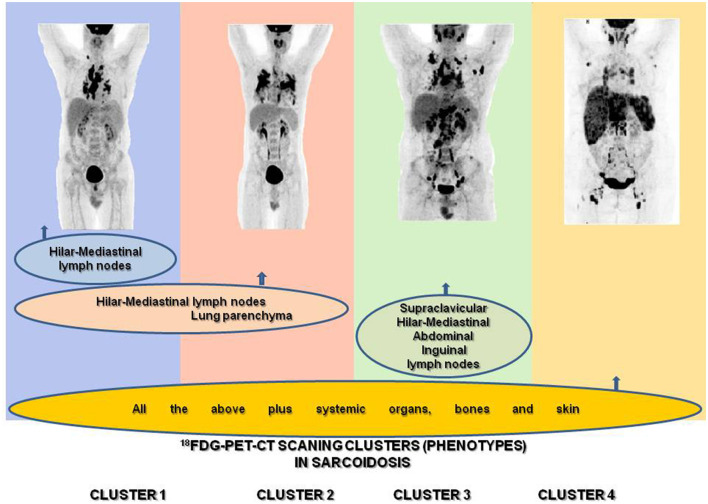
Sarcoidosis is an inflammatory granulomatous disease of unknown etiology involving any organ or tissue along with any combination of active sites, even the most silent ones clinically. The unpredictable nature of the sites involved in sarcoidosis dictates the highly variable natural history of the disease and the necessity to cluster cases at diagnosis based on clinical and/or imaging common characteristics in an attempt to classify patients based on their more homogeneous phenotypes, possibly with similar clinical behavior, prognosis, outcome, and therefore with therapeutic requirements. In the course of the disease's history, this attempt relates to the availability of a means of detection of the sites involved, from the Karl Wurm and Guy Scadding's chest x-ray staging through the ACCESS, the WASOG Sarcoidosis Organ Assessment Instruments, and the GenPhenReSa study to the F-FDG PET/CT scan phenotyping and far beyond to new technologies and/or the current "omics." The hybrid molecular imaging of the F-FDG PET/CT scan, by unveiling the glucose metabolism of inflammatory cells, can identify high sensitivity inflammatory active granulomas, the hallmark of sarcoidosis-even in clinically and physiologically silent sites-and, as recently shown, is successful in identifying an unexpected ordered stratification into four phenotypes: (I) hilar-mediastinal nodal, (II) lungs and hilar-mediastinal nodal, (III) an extended nodal supraclavicular, thoracic, abdominal, inguinal, and (IV) all the above in addition to systemic organs and tissues, which is therefore the ideal phenotyping instrument. During the "omics era," studies could provide significant, distinct, and exclusive insights into sarcoidosis phenotypes linking clinical, laboratory, imaging, and histologic characteristics with molecular signatures. In this context, the personalization of treatment for sarcoidosis patients might have reached its goal.
结节病是一种病因不明的炎症性肉芽肿疾病,可累及任何器官或组织,以及任何活动部位的组合,甚至是临床上最隐匿的部位。结节病所累及部位的不可预测性决定了该疾病高度可变的自然病程,以及在诊断时根据临床和/或影像学共同特征对病例进行聚类的必要性,以便根据患者更同质的表型进行分类,这些表型可能具有相似的临床行为、预后、结局,从而具有相似的治疗需求。在该疾病的发展历程中,这种尝试涉及检测受累部位方法的可用性,从卡尔·武尔姆(Karl Wurm)和盖伊·斯卡丁(Guy Scadding)的胸部X线分期,到ACCESS、WASOG结节病器官评估工具、GenPhenReSa研究,再到F-FDG PET/CT扫描表型分析,乃至新技术和当前的“组学”技术。F-FDG PET/CT扫描的混合分子成像通过揭示炎症细胞的葡萄糖代谢,能够识别出高敏感性的炎症性活动肉芽肿,这是结节病的标志——即使在临床和生理上隐匿的部位也是如此——并且,正如最近所显示的,成功地识别出一种意想不到的有序分层,分为四种表型:(I)肺门-纵隔淋巴结型,(II)肺部及肺门-纵隔淋巴结型,(III)广泛的锁骨上、胸部、腹部、腹股沟淋巴结型,以及(IV)除上述情况外还累及全身器官和组织型,因此这是理想的表型分析工具。在“组学时代”,研究可以为结节病表型提供重要、独特且排他的见解,将临床、实验室、影像学和组织学特征与分子特征联系起来。在这种背景下,结节病患者治疗的个性化可能已经实现了目标。