Clinic of Infectious Diseases, Department of Precision and Regenerative Medicine and Ionian Area, University of Bari, Piazza G. Cesare 11, 70124 Bari, Italy.
Hematology Unit, IRCCS Istituto Tumori "Giovanni Paolo II", 70124 Bari, Italy.
Viruses. 2023 May 19;15(5):1199. doi: 10.3390/v15051199.
Remdesivir (REM) and monoclonal antibodies (mAbs) could alleviate severe COVID-19 in at-risk outpatients. However, data on their use in hospitalized patients, particularly in elderly or immunocompromised hosts, are lacking.
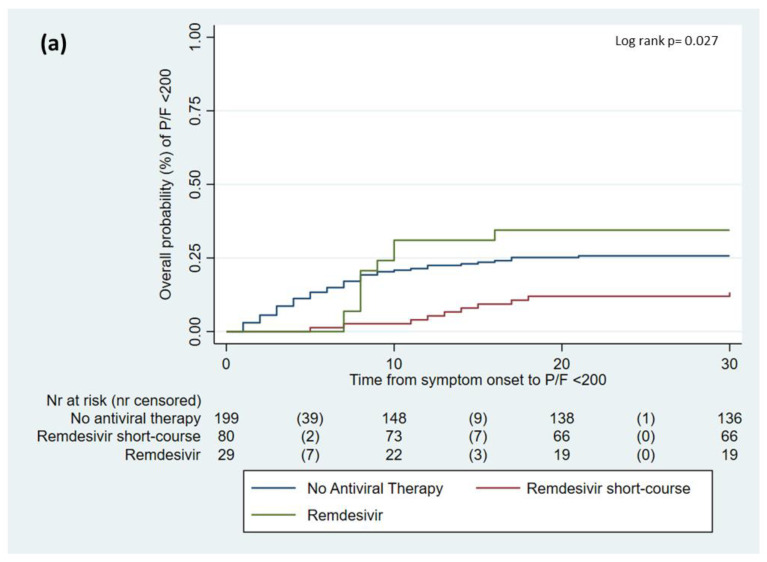
All consecutive patients hospitalized with COVID-19 at our unit from 1 July 2021 to 15 March 2022 were retrospectively enrolled. The primary outcome was the progression to severe COVID-19 (P/F < 200). Descriptive statistics, a Cox univariate-multivariate model, and an inverse probability treatment-weighted (IPTW) analysis were performed.
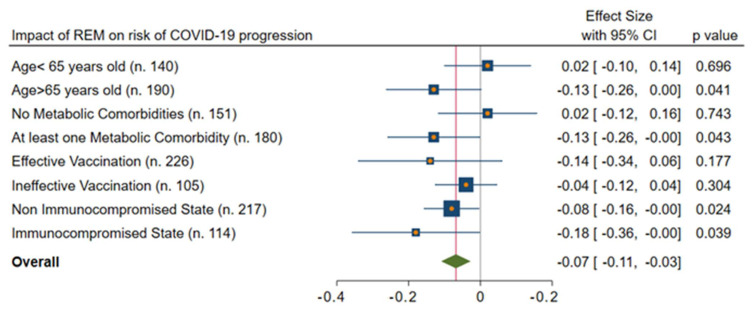
Overall, 331 subjects were included; their median (q1-q3) age was 71 (51-80) years, and they were males in 52% of the cases. Of them, 78 (23%) developed severe COVID-19. All-cause in-hospital mortality was 14%; it was higher in those with disease progression (36% vs. 7%, < 0.001). REM and mAbs resulted in a 7% (95%CI = 3-11%) and 14% (95%CI = 3-25%) reduction in the risk of severe COVID-19, respectively, after adjusting the analysis with the IPTW. In addition, by evaluating only immunocompromised hosts, the combination of REM and mAbs was associated with a significantly lower incidence of severe COVID-19 (aHR = 0.06, 95%CI = 0.02-0.77) when compared with monotherapy.
REM and mAbs may reduce the risk of COVID-19 progression in hospitalized patients. Importantly, in immunocompromised hosts, the combination of mAbs and REM may be beneficial.
瑞德西韦(Remdesivir,REM)和单克隆抗体(monoclonal antibodies,mAbs)可缓解高危门诊患者的重症 COVID-19。然而,有关其在住院患者中的应用的数据,特别是在老年或免疫功能低下宿主中的数据尚缺乏。
回顾性纳入 2021 年 7 月 1 日至 2022 年 3 月 15 日期间在我院住院的所有连续 COVID-19 患者。主要结局是进展为重症 COVID-19(P/F<200)。进行描述性统计、Cox 单变量-多变量模型和逆概率治疗加权(inverse probability treatment-weighted,IPTW)分析。
共纳入 331 例患者,中位(四分位距)年龄为 71(51-80)岁,52%为男性。其中 78 例(23%)进展为重症 COVID-19。全因院内死亡率为 14%;疾病进展患者死亡率更高(36% vs. 7%,<0.001)。在调整 IPTW 分析后,REM 和 mAbs 分别使重症 COVID-19的风险降低 7%(95%CI=3-11%)和 14%(95%CI=3-25%)。此外,仅评估免疫功能低下宿主时,与单药治疗相比,REM 和 mAbs 联合使用重症 COVID-19发生率显著降低(aHR=0.06,95%CI=0.02-0.77)。
REM 和 mAbs 可能降低住院患者 COVID-19 进展的风险。重要的是,在免疫功能低下宿主中,mAbs 和 REM 的联合治疗可能有益。