Fitzsimmons Timothy S, Singh Niharika, Walker Thomas D J, Newton Claire, Evans Dafydd G R, Crosbie Emma J, Ryan Neil A J
Clinical Medical School, University of Bristol, Bristol, United Kingdom.
Division of Cancer Sciences, St Mary's Hospital, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, United Kingdom.
Front Med (Lausanne). 2023 May 12;10:1192762. doi: 10.3389/fmed.2023.1192762. eCollection 2023.
Immune checkpoint inhibitors (ICPI) are a tumor agnostic treatment. However, trials of their use have been site specific. Here we summarize the trial data and explore the utility of programmed death-ligand 1 (PD-L1) expression as a biomarker to direct their pan-cancer use.
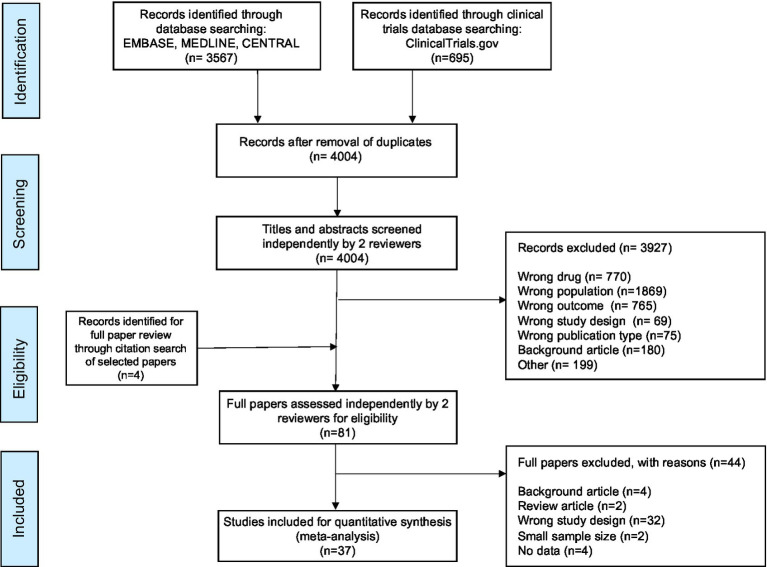
A systematic review of literature, following PRISMA guidelines, was performed. Medline, Embase, Cochrane CENTRAL, NHS Health and Technology, and Web of Science were searched from their conception to June 2022 limited to the English language. The search terms and method were devised by a specialist medical librarian. Studies were limited to adults with solid cancers (excluding melanomas) treated with ICPIs. Only phase III randomized control trials (RCT) were included. The primary outcome was overall survival and secondary outcomes were progression free survival, PD-L1 expression, quality of life outcomes and adverse event data. Where present in eligible clinical trials, hazard ratios (HR), risk ratios (RR), standard error (SE) and 95% confidence intervals (CI) were extracted or calculated. Heterogeneity across studies was described with the use of an score (Low: 25, 50%: moderate, 75% low heterogeneity). HR pools inverse variance methods were adopted by Random Effects (RE). Means were standardized across any heterogenous scale limits.
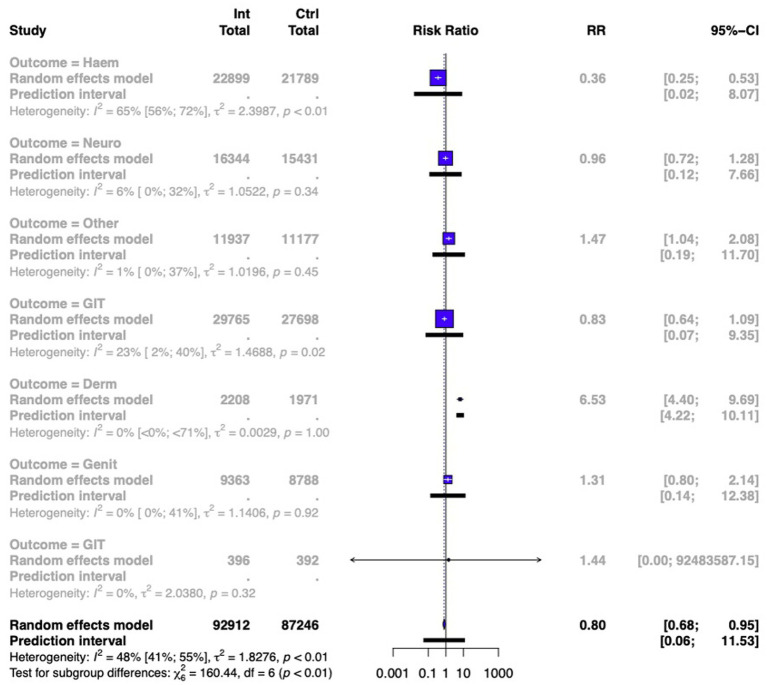
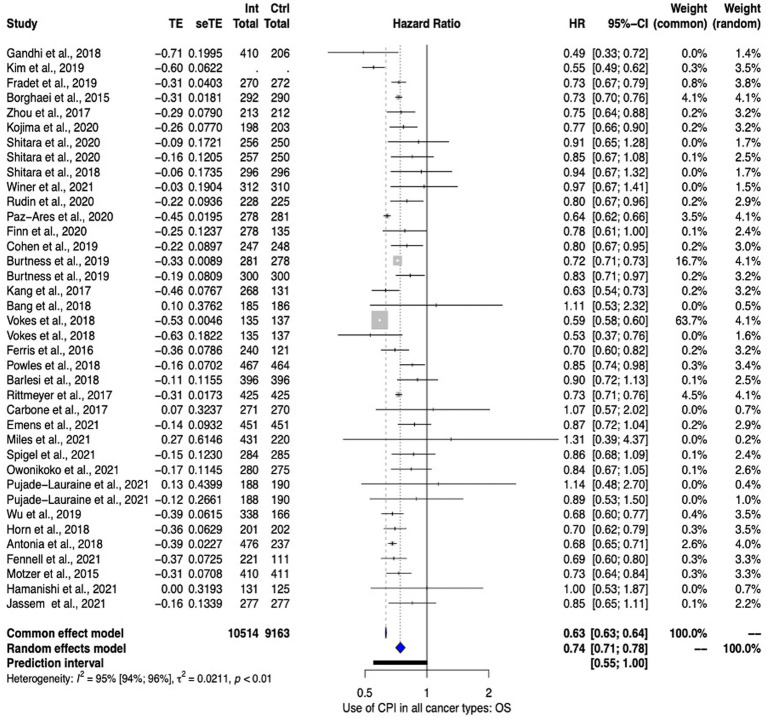
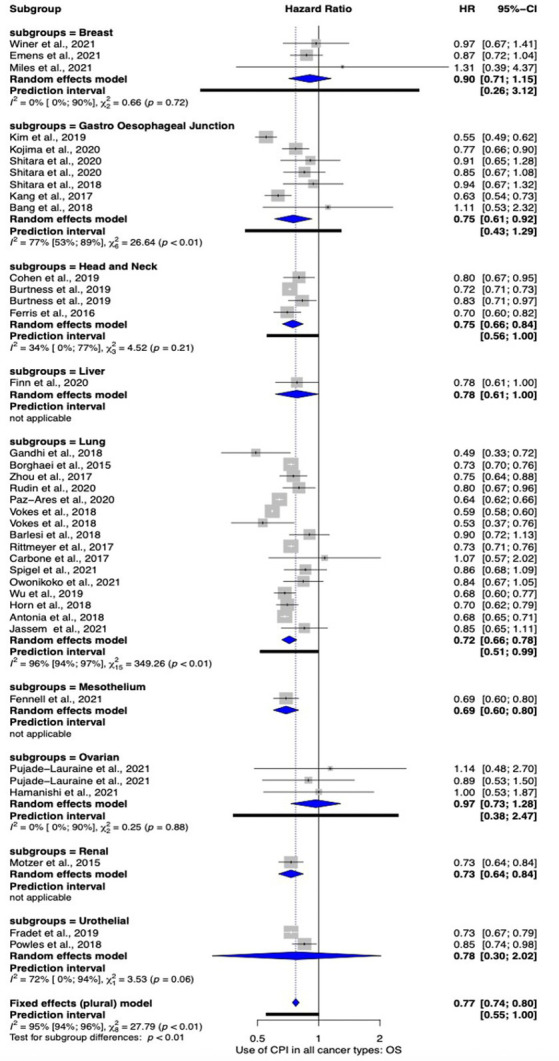
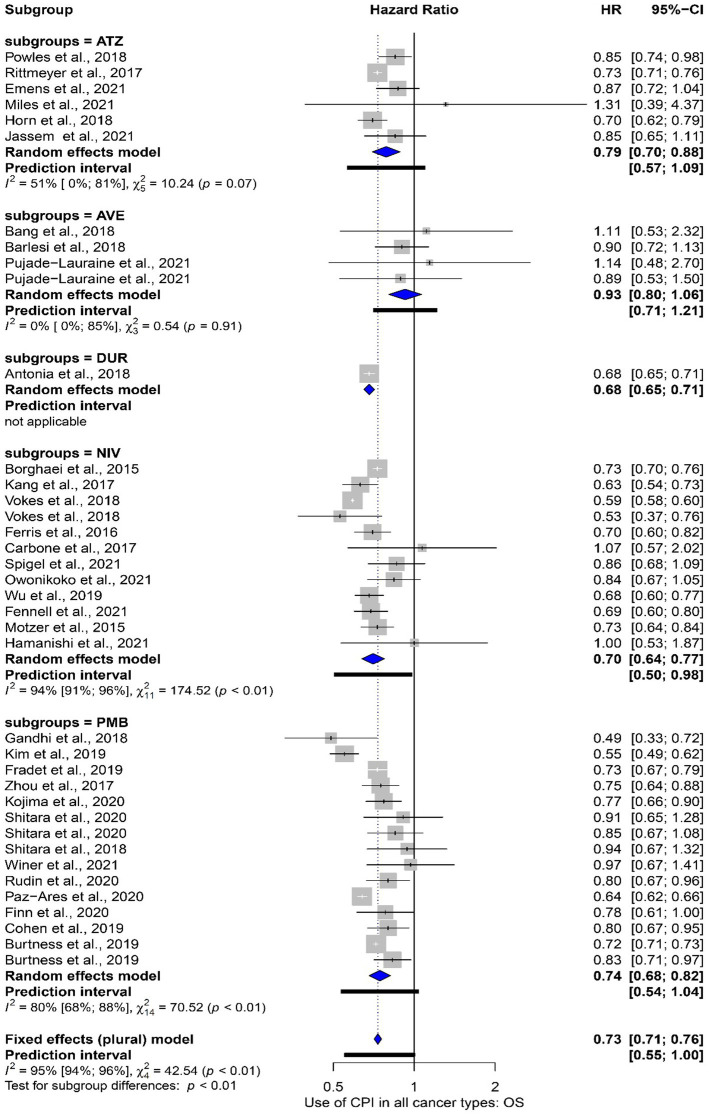
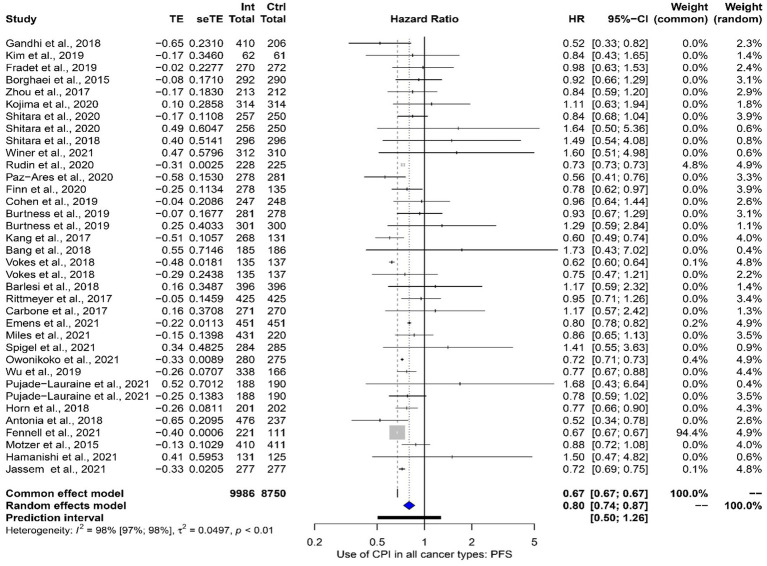
In total 46,510 participants were included in the meta-analysis. Overall, meta-analysis favored the use of ICPIs with an overall survival (OS) HR of 0.74 (95% CI 0.71 to 0.78). Lung cancers showed the most benefit in OS [HR 0.72 (95% 0.66-0.78)] followed by head and neck cancers [HR 0.75 (95% CI 0.66-0.84)] and gastroesophageal junction cancers [HR 0.75 (95% CI 0.61-0.92)]. ICPIs seem to be efficacious at both primary presentation and recurrence [OS HR 0.73 (95% CI 0.68-0.77)] vs. [OS HR 0.79 (95% CI 0.72 to 0.87)] respectively. Interestingly, subgroup analysis comparing studies in which most cancers demonstrated PD-L1 expression vs. those studies in which a minority of cancer demonstrated PD-L1 expression reported similar effect of ICPI use on OS; oddly the data favored ICPI use in studies with a minority of PD-L1 expression. Specifically, studies with minority PD-L1 expression had an HR 0.73 (95% CI 0.68-0.78) vs. studies with majority PD-L1 expression HR 0.76 (95% CI 0.70-0.84). This was maintained even when studies exploring the same cancer site were directly compared. Subgroup analysis was performed comparing the impact on OS subdivided by the specific ICPI used. Where meta-analysis was performed, Nivolumab led to the greatest impact [HR 0.70 (95% CI 0.64-0.77)] with Avelumab failing to reach significance [HR 0.93 (95% CI 0.80-1.06)]. However, overall heterogenicity was high ( = 95%). Finally, the use of ICPIs led to an improved side effect profile when compared with standard chemotherapy [RR 0.85 (95% CI 0.73-0.98)].
ICPIs improve survival outcomes in all cancer types. These effects are seen in the primary, recurrent, chemotherapy sensitive, chemotherapy resistant disease. These data support their use as a tumor agnostic therapy. Furthermore, they are well tolerated. However, PD-L1 as a biomarker for the targeting of ICPI use seems problematic. Other biomarkers such as mismatch repair or tumor mutational burden should be explored in randomized trials. In addition, there are still limited trials looking at ICPI use outside of lung cancer.
免疫检查点抑制剂(ICPI)是一种不针对特定肿瘤类型的治疗方法。然而,其使用试验是针对特定部位的。在此,我们总结试验数据,并探讨程序性死亡配体1(PD-L1)表达作为生物标志物指导其在泛癌治疗中应用的效用。
按照PRISMA指南对文献进行系统综述。检索了Medline、Embase、Cochrane CENTRAL、NHS Health and Technology以及Web of Science数据库,检索时间从建库至2022年6月,限定语言为英语。检索词和方法由专业医学图书馆员设计。研究限于接受ICPI治疗的实体癌(不包括黑色素瘤)成年患者。仅纳入III期随机对照试验(RCT)。主要结局为总生存期,次要结局为无进展生存期、PD-L1表达、生活质量结局和不良事件数据。在符合条件的临床试验中,提取或计算风险比(HR)、风险率(RR)、标准误(SE)和95%置信区间(CI)。使用I²评分描述研究间的异质性(低:I²<25%,中度:25%≤I²<50%,高度:I²≥50%)。采用随机效应(RE)的HR合并逆方差方法。对任何异质性量表范围进行均值标准化。
荟萃分析共纳入46510名参与者。总体而言,荟萃分析支持使用ICPI,总生存期(OS)的HR为0.74(95%CI 0.71至0.78)。肺癌在OS方面获益最大[HR 0.72(95%CI 0.66 - 0.78)],其次是头颈癌[HR 0.75(95%CI 0.66 - 0.84)]和胃食管交界癌[HR 0.75(95%CI 0.61 - 0.92)]。ICPI在初次治疗和复发时似乎均有效[OS HR 0.73(95%CI 0.68 - 0.77)]与[OS HR 0.79(95%CI 0.72至0.87)]。有趣的是,亚组分析比较了大多数癌症显示PD-L1表达的研究与少数癌症显示PD-L1表达的研究,结果显示ICPI使用对OS的影响相似;奇怪的是,数据支持在少数PD-L1表达的研究中使用ICPI。具体而言,少数PD-L1表达的研究HR为0.73(95%CI 0.68 - 0.78),而多数PD-L1表达的研究HR为0.76(95%CI 0.70 - 0.84)。即使直接比较同一癌症部位的研究,这一结果仍然成立。进行亚组分析以比较不同特定ICPI对OS的影响。进行荟萃分析的结果中,纳武单抗产生的影响最大[HR 0.70(95%CI 0.64 - 0.77)],阿维鲁单抗未达到显著差异[HR 0.93(95%CI 0.80 - 1.06)]。然而,总体异质性较高(I² = 95%)。最后,与标准化疗相比,ICPI的使用导致副作用情况改善[RR = 0.85(95%CI 0.73 - 0.98)]。
ICPI可改善所有癌症类型的生存结局。在原发性、复发性、化疗敏感和化疗耐药疾病中均可见到这些效果。这些数据支持将其用作不针对特定肿瘤类型的治疗方法。此外,它们耐受性良好。然而,PD-L1作为指导ICPI使用的生物标志物似乎存在问题。应在随机试验中探索其他生物标志物,如错配修复或肿瘤突变负荷。此外,研究ICPI在肺癌以外应用的试验仍然有限。