Department of Endocrinology and Diabetes, Clinic for Diabetology, Department of Internal Medicine, Medical University Graz, Graz, Austria.
Daiichi Sankyo Europe GmbH, Munich, Germany.
Wien Klin Wochenschr. 2023 Jul;135(13-14):364-374. doi: 10.1007/s00508-023-02221-4. Epub 2023 Jun 8.
The low-density lipoprotein cholesterol goals in the 2019 European Society of Cardiology/European Atherosclerosis Society dyslipidaemia guidelines necessitate greater use of combination therapies. We describe a real-world cohort of patients in Austria and simulate the addition of oral bempedoic acid and ezetimibe to estimate the proportion of patients reaching goals.
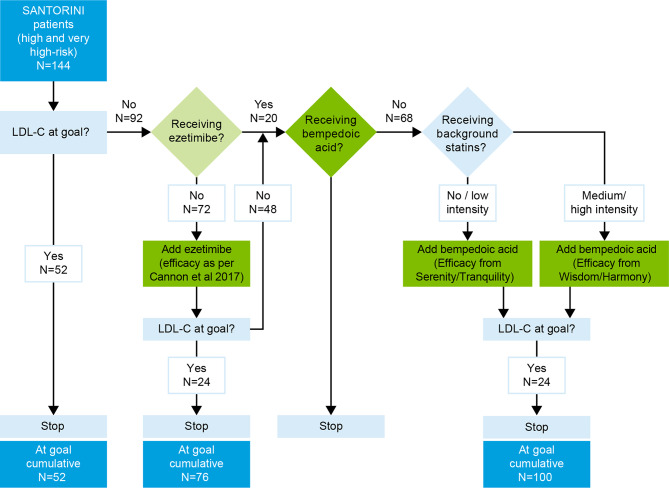
Patients at high or very high cardiovascular risk on lipid-lowering treatments (excluding proprotein convertase subtilisin/kexin type 9 inhibitors) from the Austrian cohort of the observational SANTORINI study were included using specific criteria. For patients not at their risk-based goals at baseline, addition of ezetimibe (if not already received) and subsequently bempedoic acid was simulated using a Monte Carlo simulation.
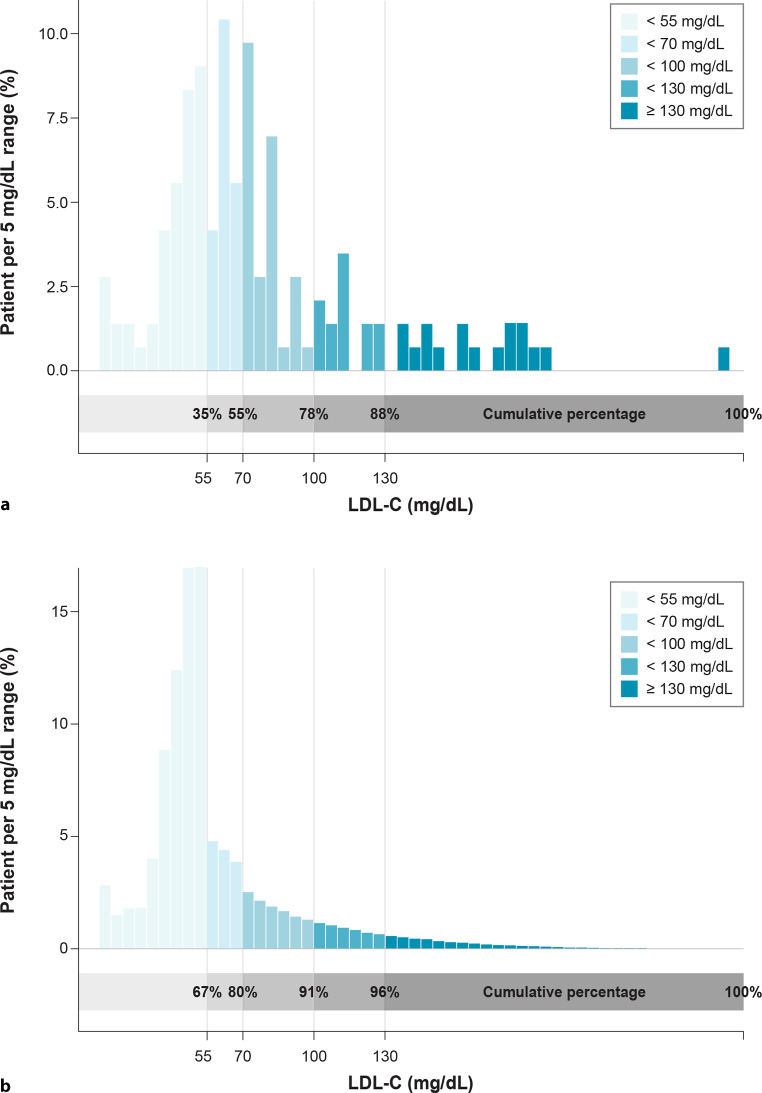
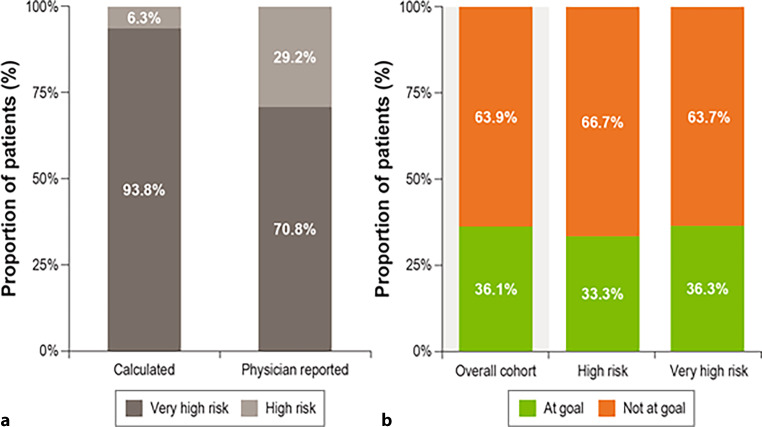
A cohort of patients (N = 144) with a mean low-density lipoprotein cholesterol of 76.4 mg/dL, with 94% (n = 135) on statins and 24% (n = 35) on ezetimibe monotherapy or in combination, were used in the simulation. Only 36% of patients were at goal (n = 52). Sequential simulation of ezetimibe (where applicable) and bempedoic acid increased the proportion of patients at goal to 69% (n = 100), with a decrease in the mean low-density lipoprotein cholesterol from 76.4 mg/dL at baseline to 57.7 mg/dL overall.
The SANTORINI real-world data in Austria suggest that a proportion of high and very high-risk patients remain below the guideline-recommended low-density lipoprotein cholesterol goals. Optimising use of oral ezetimibe and bempedoic acid after statins in the lipid-lowering pathway could result in substantially more patients attaining low-density lipoprotein cholesterol goals, likely with additional health benefits.
2019 年欧洲心脏病学会/欧洲动脉粥样硬化学会血脂异常指南中的低密度脂蛋白胆固醇目标需要更多地使用联合治疗。我们描述了奥地利真实世界队列中的患者,并模拟添加口服贝匹地酸和依折麦布,以估计达到目标的患者比例。
使用特定标准纳入降脂治疗(不包括前蛋白转化酶枯草溶菌素/克那霉 9 抑制剂)中处于高或极高心血管风险的奥地利 SANTORINI 观察性研究队列中的患者。对于基线时未达到风险目标的患者,如果未接受依折麦布(如果未接受),则使用蒙特卡罗模拟模拟添加贝匹地酸。
我们使用了一个平均 LDL-C 为 76.4mg/dL 的患者队列(N=144),其中 94%(n=135)接受他汀类药物治疗,24%(n=35)接受依折麦布单药或联合治疗。只有 36%的患者达到目标(n=52)。依折麦布(如有适用)和贝匹地酸的序贯模拟将达到目标的患者比例增加到 69%(n=100),总体 LDL-C 从基线时的 76.4mg/dL 降至 57.7mg/dL。
奥地利 SANTORINI 真实世界数据表明,一部分高危和极高危患者的 LDL-C 仍低于指南推荐的目标。在降脂途径中优化使用他汀类药物后口服依折麦布和贝匹地酸可能会使更多的患者达到 LDL-C 目标,可能会带来更多的健康益处。