Sagar Kelly A, Dahlgren M Kathryn, Smith Rosemary T, Lambros Ashley M, Gruber Staci A
Cognitive and Clinical Neuroimaging Core (CCNC), McLean Hospital, Belmont, MA, USA.
Marijuana Investigations for Neuroscientific Discovery (MIND) Program, McLean Hospital, Belmont, MA, USA.
Cannabis. 2021 Oct 1;4(2):47-59. doi: 10.26828/cannabis/2021.02.004. eCollection 2021.
To date, no studies have directly assessed potential cannabis use disorder (CUD) in medical cannabis (MC) patients pre- vs post-MC treatment. Given that MC patients use cannabis for symptom alleviation rather than intoxication, we hypothesized that MC patients would exhibit few symptoms of CUD after initiating MC treatment.
As part of an ongoing observational, longitudinal study, 54 MC patients completed baseline assessments prior to initiating MC use and returned for at least one follow-up assessment after three, six, and/or twelve months of a self-selected MC treatment regimen; detailed MC treatment information was collected and quantified. All patients completed the Cannabis Use Disorder Identification Test - Revised (CUDIT-R) at each visit. Changes in individual items scores and total scores were assessed over time, and we examined whether total CUDIT-R scores correlated with frequency of MC use, delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) exposure. Further, Cronbach's alpha analyses were conducted to provide preliminary data regarding the psychometric properties of the CUDIT-R when used among MC patients.
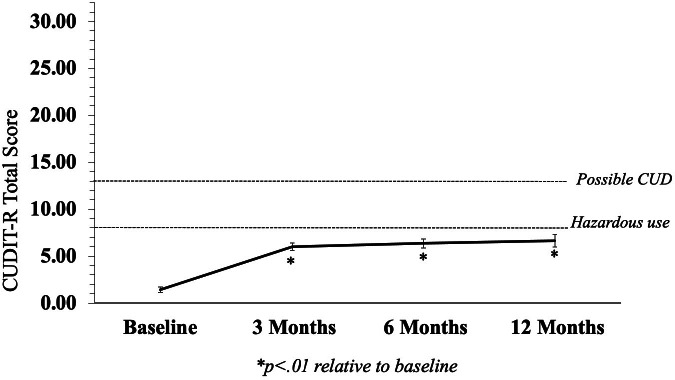
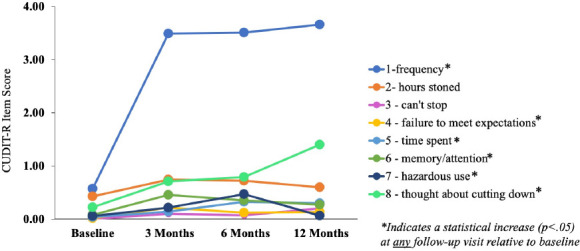
Although total CUDIT-R scores increased relative to baseline, on average, ratings fell below the 'hazardous use' threshold at each visit. Analyses of individual items revealed that increases in total scores were primarily attributable to increases in frequency of use and not necessarily other aspects of problematic use. Total CUDIT-R scores were not associated with number of MC uses or CBD exposure, but a significant relationship was detected between increased THC exposure and higher CUDIT-R scores. Importantly however, analyses revealed that the CUDIT-R does not appear to be an appropriate tool for identifying CUD in MC patients.
Screening tools specifically designed to assess CUD in MC patients are needed and should distinguish between frequent use and problematic use; exposure to individual cannabinoids must also be considered.
迄今为止,尚无研究直接评估医用大麻(MC)患者在接受MC治疗前后的潜在大麻使用障碍(CUD)情况。鉴于MC患者使用大麻是为了缓解症状而非追求成瘾,我们推测MC患者在开始MC治疗后CUD症状会很少。
作为一项正在进行的观察性纵向研究的一部分,54名MC患者在开始使用MC之前完成了基线评估,并在自行选择的MC治疗方案进行3个月、6个月和/或12个月后返回进行至少一次随访评估;收集并量化了详细的MC治疗信息。所有患者在每次就诊时均完成修订版大麻使用障碍识别测试(CUDIT-R)。评估了各个项目得分和总分随时间的变化,并且我们研究了CUDIT-R总分是否与MC使用频率、Δ-9-四氢大麻酚(THC)和大麻二酚(CBD)暴露量相关。此外,进行了克朗巴哈系数分析,以提供关于CUDIT-R在MC患者中使用时心理测量特性的初步数据。
尽管CUDIT-R总分相对于基线有所增加,但平均而言,每次就诊时的评分均低于“危险使用”阈值。对各个项目的分析表明,总分的增加主要归因于使用频率的增加,而不一定是问题使用的其他方面。CUDIT-R总分与MC使用次数或CBD暴露量无关,但在THC暴露量增加与较高的CUDIT-R得分之间检测到显著关系。然而,重要的是,分析表明CUDIT-R似乎不是识别MC患者中CUD的合适工具。
需要专门设计用于评估MC患者中CUD的筛查工具,并且该工具应区分频繁使用和问题使用;还必须考虑个体大麻素的暴露情况。