Huang Dan, Vithran Djandan Tadum Arthur, Gong Hao-Li, Zeng Ming, Tang Zhong-Wen, Rao Zhou-Zhou, Wen Jie, Xiao Sheng
Department of Pediatric Orthopedics, Hunan Provincial People's Hospital, The First Affiliated Hospital of Hunan Normal University, Changsha 410013, Hunan Province, China.
Department of Orthopaedics, Xiangya Hospital of Central South University, Changsha 410013, Hunan Province, China.
World J Orthop. 2023 Jun 18;14(6):485-501. doi: 10.5312/wjo.v14.i6.485.
The effectiveness of Platelet-Rich Plasma (PRP) in the treatment of patients with Achilles tendon rupture (ATR) and Achilles tendinopathy (AT) has been controversial.
To assess PRP injections' effectiveness in treating ATR and AT.
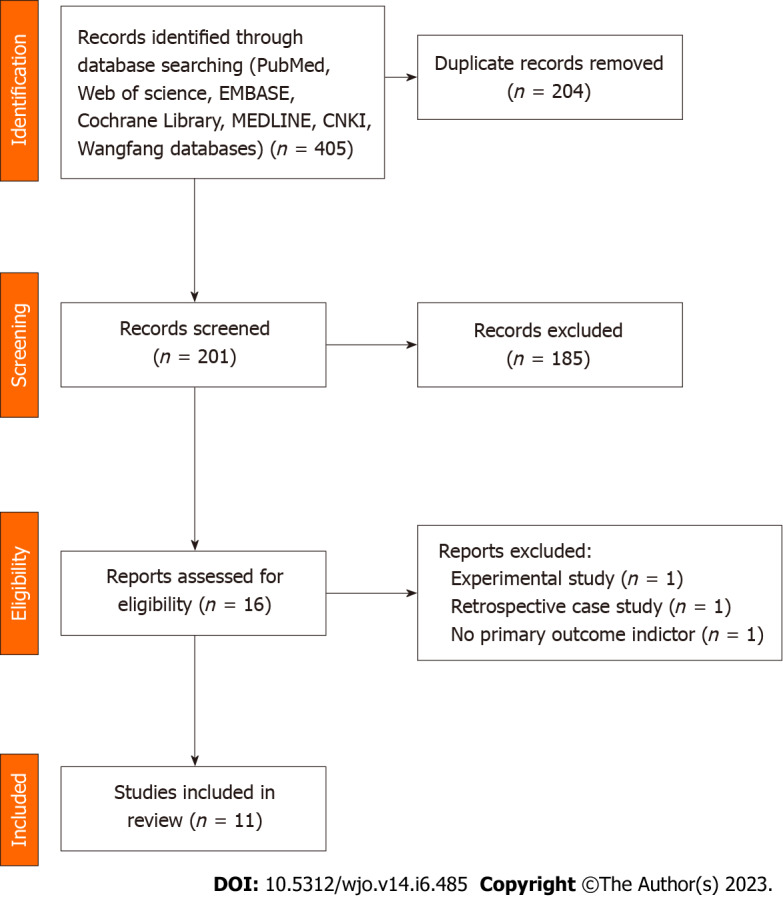
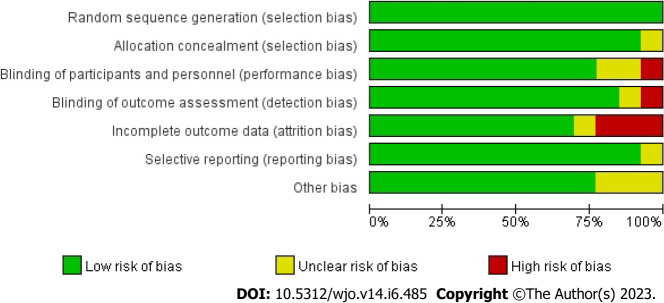
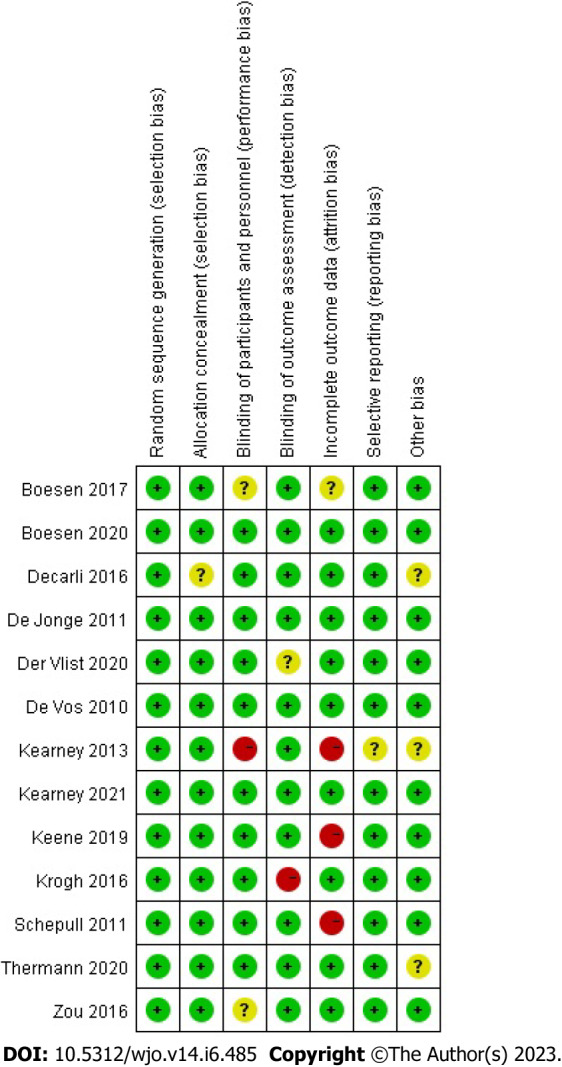
A comprehensive review of relevant literature was conducted utilizing multiple databases such as Cochrane Library, PubMed, Web of Science, Chinese Science and Technology Journal, EMBASE, and China Biomedical CD-ROM. The present investigation integrated randomized controlled trials that assessed the effectiveness of platelet-rich plasma injections in managing individuals with Achilles tendon rupture and tendinopathy. The eligibility criteria for the trials encompassed publications that were published within the timeframe of January 1, 1966 to December 2022. The statistical analysis was performed utilizing the Review Manager 5.4.1, the visual analogue scale (VAS), Victorian Institute Ankle Function Scale (VISA-A), and Achilles Tendon Thickness were used to assess outcomes.
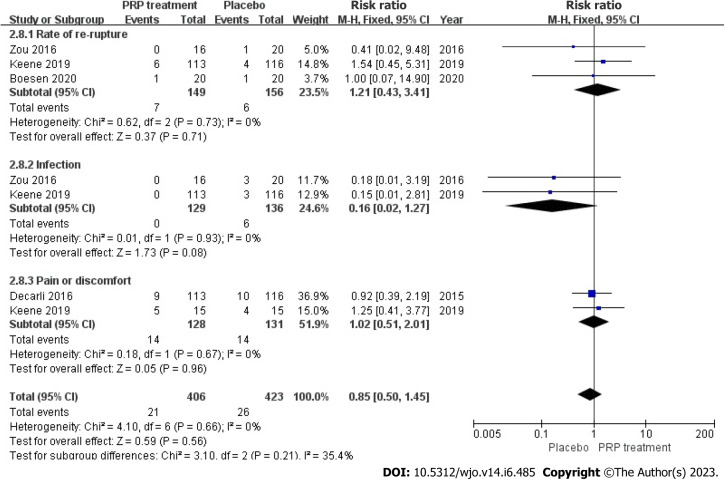
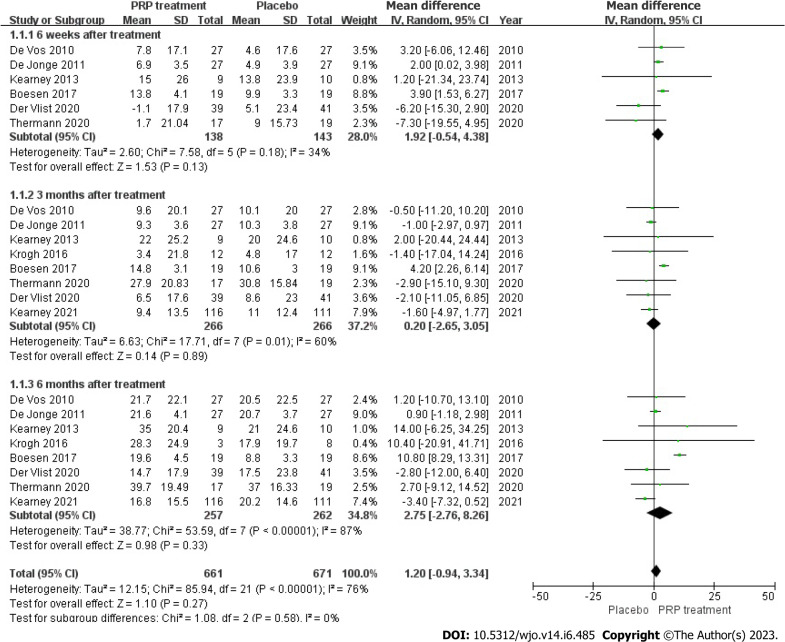
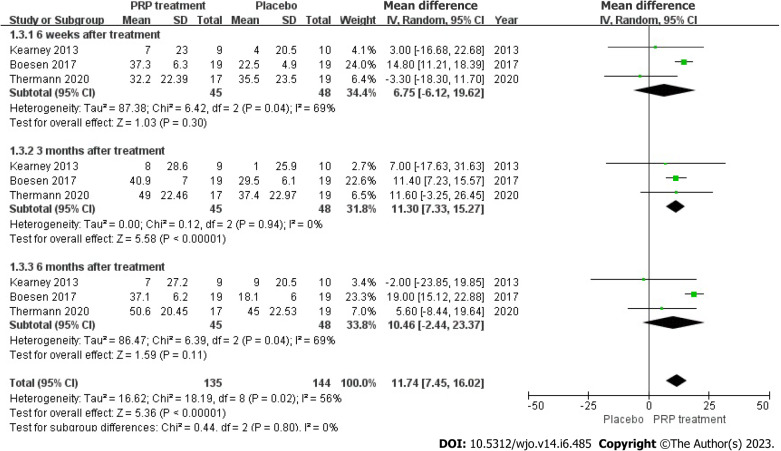
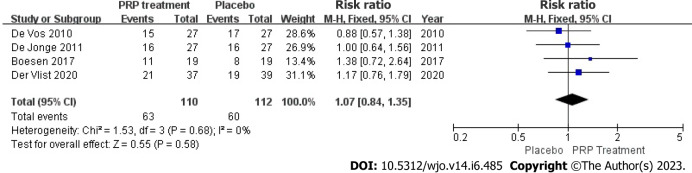
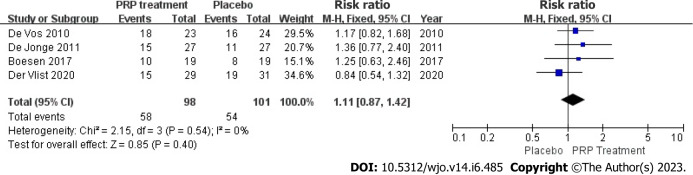
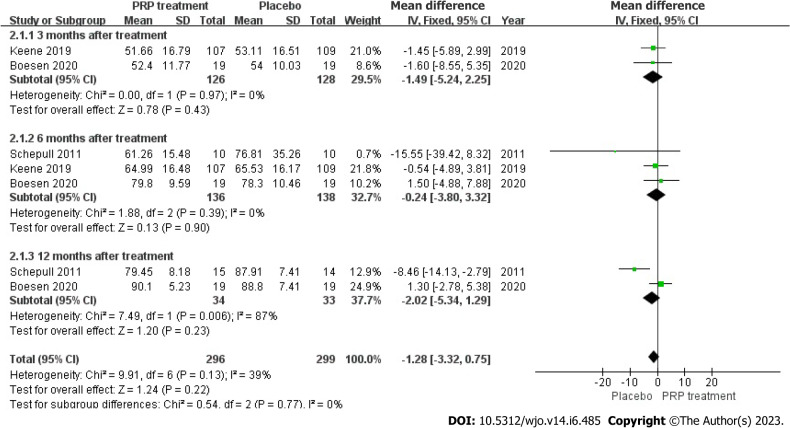
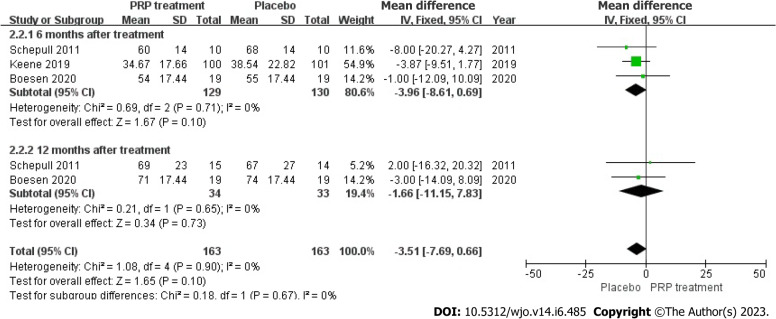
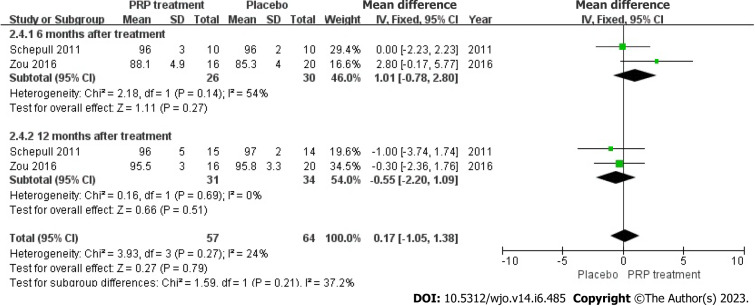
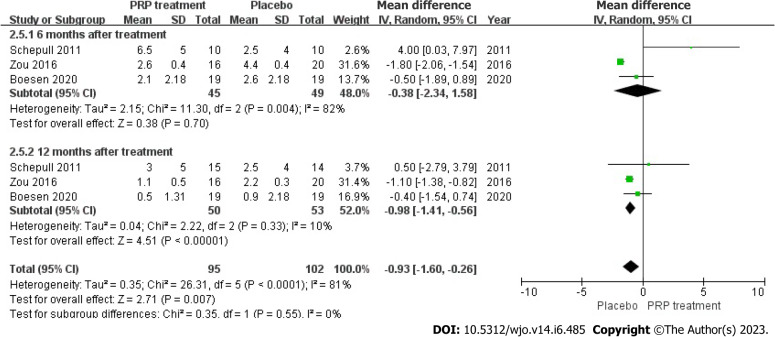
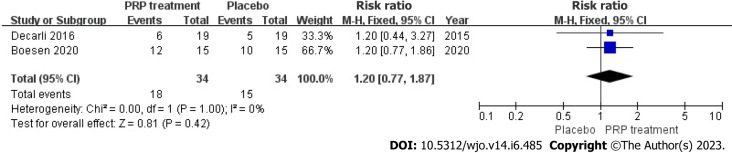
This meta-analysis included 13 randomized controlled trials, 8 of which were randomized controlled trials of PRP for AT and 5 of which were randomized controlled trials of PRP for ATR. PRP for AT at 6 wk [weighted mean difference (WMD) = 1.92, 95%CI: -0.54 to 4.38, = 34%], at 3 mo [WMD = 0.20, 95%CI: -2.65 to 3.05, = 60%], and 6 mo [WMD = 2.75, 95%CI: -2.76 to 8.26, = 87%) after which there was no significant difference in VISA-A scores between the PRP and control groups. There was no significant difference in VAS scores between the PRP group and the control group after 6 wk [WMD = 6.75, 95%CI: -6.12 to 19.62, = 69%] and 6 mo [WMD = 10.46, 95%CI: -2.44 to 23.37, = 69%] of treatment, and at mid-treatment at 3 mo [WMD = 11.30, 95%CI: 7.33 to 15.27, = 0%] after mid-treatment, the PRP group demonstrated better outcomes than the control group. Post-treatment patient satisfaction [WMD = 1.07, 95%CI: 0.84 to 1.35, = 0%], Achilles tendon thickness [WMD = 0.34, 95%CI: -0.04 to 0.71, = 61%] and return to sport [WMD = 1.11, 95%CI: 0.87 to 1.42, = 0%] were not significantly different between the PRP and control groups. The study did not find any statistically significant distinction between the groups that received PRP treatment and those that did not, regarding the Victorian Institute of Sport Assessment - Achilles scores at 3 mo [WMD = -1.49, 95%CI: -5.24 to 2.25, = 0%], 6 mo [WMD = -0.24, 95%CI: -3.80 to 3.32, = 0%], and 12 mo [WMD = -2.02, 95%CI: -5.34 to 1.29, = 87%] for ATR patients. Additionally, no significant difference was observed between the PRP and the control groups in improving Heel lift height respectively at 6 mo [WMD = -3.96, 95%CI: -8.61 to 0.69, = 0%] and 12 mo [WMD = -1.66, 95%CI: -11.15 to 7.83, = 0%] for ATR patients. There was no significant difference in calf circumference between the PRP group and the control group after 6 mo [WMD = 1.01, 95%CI: -0.78 to 2.80, = 54%] and 12 mo [WMD = -0.55, 95%CI: -2.2 to 1.09, = 0%] of treatment. There was no significant difference in ankle mobility between the PRP and control groups at 6 mo of treatment [WMD = -0.38, 95%CI: -2.34 to 1.58, = 82%] and after 12 mo of treatment [WMD = -0.98, 95%CI: -1.41 to -0.56, = 10%] there was a significant improvement in ankle mobility between the PRP and control groups. There was no significant difference in the rate of return to exercise after treatment [WMD = 1.20, 95%CI: 0.77 to 1.87, = 0%] and the rate of adverse events [WMD = 0.85, 95%CI: 0.50 to 1.45, = 0%] between the PRP group and the control group.
The use of PRP for AT improved the patient's immediate VAS scores but not VISA-A scores, changes in Achilles tendon thickness, patient satisfaction, or return to sport. Treatment of ATR with PRP injections alone improved long-term ankle mobility but had no significant effect on VISA-A scores, single heel lift height, calf circumference or return to sport. Additional research employing more extensive sampling sizes, more strict experimental methods, and standard methodologies may be necessary to yield more dependable and precise findings.
富血小板血浆(PRP)在治疗跟腱断裂(ATR)和跟腱病(AT)患者中的有效性一直存在争议。
评估PRP注射治疗ATR和AT的有效性。
利用多个数据库进行相关文献的全面综述,这些数据库包括Cochrane图书馆、PubMed、科学网、中国科技期刊、EMBASE和中国生物医学光盘数据库。本研究纳入了评估富血小板血浆注射治疗跟腱断裂和跟腱病患者有效性的随机对照试验。试验的纳入标准包括1966年1月1日至2022年12月期间发表的文献。使用Review Manager 5.4.1进行统计分析,采用视觉模拟量表(VAS)、维多利亚踝关节功能量表(VISA - A)和跟腱厚度来评估结果。
该荟萃分析包括13项随机对照试验,其中8项是PRP治疗AT的随机对照试验,5项是PRP治疗ATR 的随机对照试验。PRP治疗AT在6周时[加权平均差(WMD)=1.92,95%置信区间:-0.54至4.38,I² = 34%],3个月时[WMD = 0.20,95%置信区间:-2.65至3.05,I² = 60%],6个月时[WMD = 2.75,95%置信区间:-2.76至8.26,I² = 87%]后,PRP组和对照组之间的VISA - A评分无显著差异。治疗6周[WMD = 6.75,95%置信区间:-6.12至19.62,I² = 69%]和6个月[WMD = 10.46,95%置信区间:-2.44至23.37,I² = 69%]后,PRP组和对照组之间的VAS评分无显著差异,在治疗3个月中期[WMD = 11.30,95%置信区间:7.33至15.27,I² = 0%]时,PRP组的结果优于对照组。治疗后患者满意度[WMD = 1.07,95%置信区间:0.84至1.35,I² = 0%]、跟腱厚度[WMD = 0.34,95%置信区间:-0.04至0.71,I² = 61%]和恢复运动情况[WMD = 1.11,95%置信区间:0.87至1.42,I² = 0%]在PRP组和对照组之间无显著差异。该研究未发现接受PRP治疗的组与未接受PRP治疗的组在3个月[WMD = -1.49,95%置信区间:-5.24至2.25,I² = 0%]、6个月[WMD = -0.24,95%置信区间:-3.80至3.32,I² = 0%]和12个月[WMD = -2.02,95%置信区间:-5.34至1.29,I² = 87%]时的维多利亚运动评估 - 跟腱评分上有任何统计学显著差异。此外,对于ATR患者,在6个月[WMD = -3.96,95%置信区间:-8.61至0.69,I² = 0%]和12个月[WMD = -1.66,95%置信区间:-11.15至7.83,I² = 0%]时,PRP组和对照组在提高足跟抬起高度方面无显著差异。治疗6个月[WMD = 1.01,95%置信区间:-0.78至2.80,I² = 54%]和12个月[WMD = -0.55,95%置信区间:-2.2至1.09,I² = 0%]后,PRP组和对照组之间的小腿围度无显著差异。治疗6个月时PRP组和对照组之间的踝关节活动度无显著差异[WMD = -0.38,95%置信区间:-2.34至1.58,I² = 82%],治疗12个月后PRP组和对照组之间的踝关节活动度有显著改善[WMD = -0.98,95%置信区间:-1.41至-0.56,I² = 10%]。PRP组和对照组在治疗后恢复运动率[WMD = 1.20,95%置信区间:0.77至1.87,I² = 0%]和不良事件发生率[WMD = 0.85,95%置信区间:0.50至1.45,I² = 0%]方面无显著差异。
PRP用于治疗AT可改善患者的即时VAS评分,但对VISA - A评分、跟腱厚度变化、患者满意度或恢复运动情况无改善作用。单独使用PRP注射治疗ATR可改善长期踝关节活动度,但对VISA - A评分、单足跟抬起高度、小腿围度或恢复运动情况无显著影响。可能需要采用更大样本量、更严格的实验方法和标准方法进行更多研究,以得出更可靠和精确的结果。