Alifu Muyesar, Tao Min, Chen Xiao, Chen Jie, Tang Kejing, Tang Yubo
Department of Pharmacy, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China.
Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China.
Front Oncol. 2023 Jun 15;13:1146905. doi: 10.3389/fonc.2023.1146905. eCollection 2023.
Recent clinical trials have confirmed that anti-programmed cell death-1/ligand 1 (anti-PD-1/L1) combined with either anti-cytotoxic T-lymphocyte-associated protein 4 (anti-CTLA-4) or anti-T-cell immunoreceptor with Ig and ITIM domains (TIGIT) antibodies (dual immunotherapy) produced significant benefits as first-line therapies for patients with advanced non-small cell lung cancer (NSCLC). However, it also increased the incidence of adverse reactions, which cannot be ignored. Our study aims to explore the efficacy and safety of dual immunotherapies in advanced NSCLC.
This meta-analysis ultimately included nine first-line randomized controlled trials collected from PubMed, EMBASE, and Cochrane Central Register of Controlled Trials databases until 13 August 2022. Efficacy was measured as the hazard ratio (HR) and 95% confidence interval (CI) for progression-free survival (PFS), overall survival (OS), and risk ratio (RR) for the objective response rates (ORRs). Treatment safety was assessed by RR of any grade of treatment-related adverse events (TRAEs) and grade ≥ 3 TRAEs.
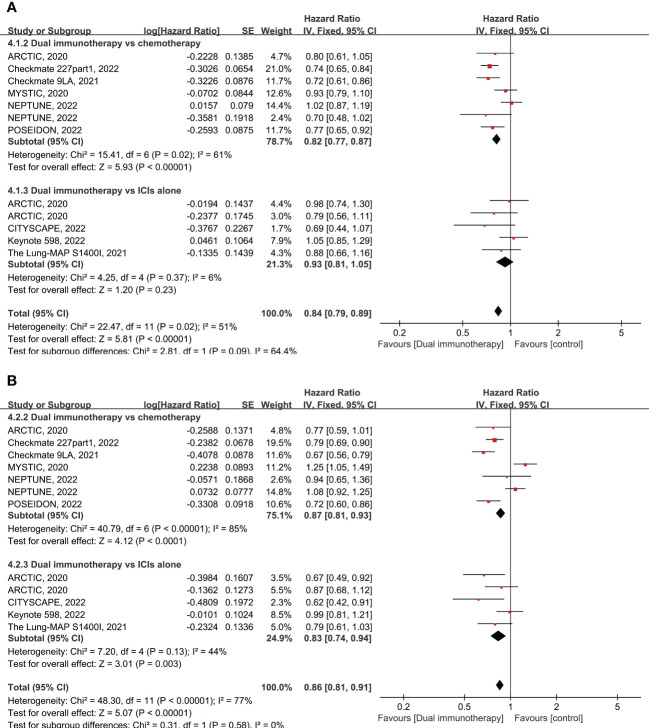
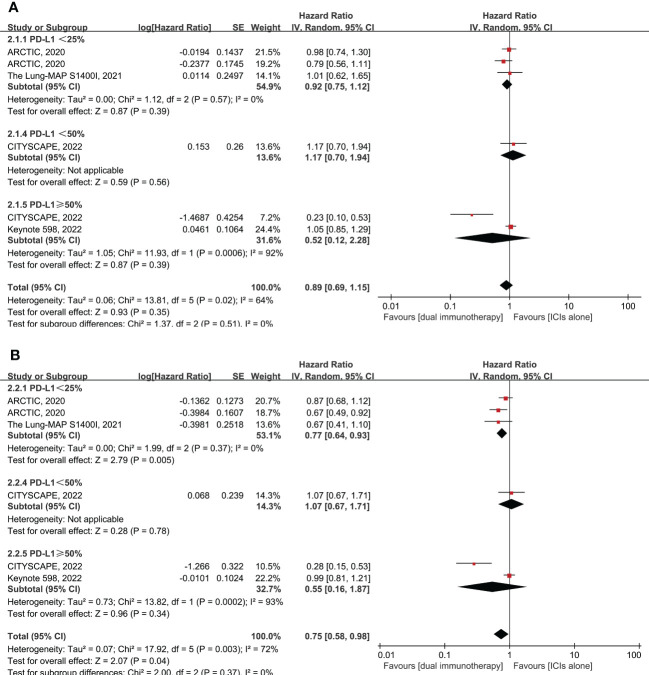
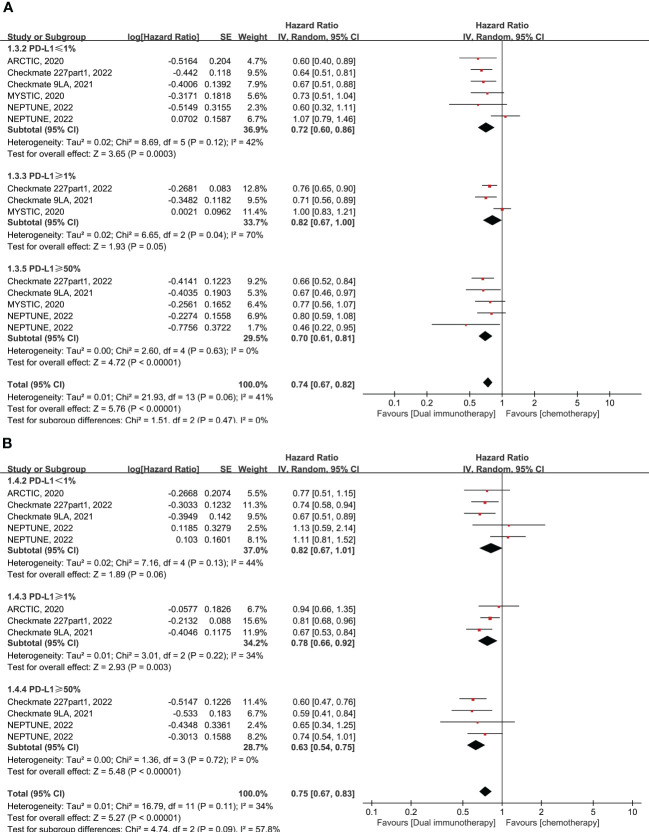
Our results demonstrated that, compared to chemotherapy, dual immunotherapy shows durable benefits in OS (HR = 0.76, 95% CI: 0.69-0.82) and PFS (HR = 0.75, 95% CI: 0.67-0.83) across all levels of PD-L1 expression. Subgroup analysis also presented that dual immunotherapy resulted in improved long-term survival compared with chemotherapy in patients with a high tumor mutational burden (TMB) (OS: HR = 0.76, = 0.0009; PFS: HR = 0.72, < 0.0001) and squamous cell histology (OS: HR = 0.64, < 0.00001; PFS: HR = 0.66, < 0.001). However, compared with immune checkpoint inhibitor (ICI) monotherapy, dual immunotherapy shows some advantages in terms of OS and ORR and only improved PFS (HR = 0.77, = 0.005) in PD-L1 < 25%. With regard to safety, there was no significant difference in any grade TRAEs ( = 0.05) and grade ≥ 3 TRAEs ( = 0.31) between the dual immunotherapy and chemotherapy groups. However, compared with ICI monotherapy, dual immunotherapy significantly increased the incidence of any grade TRAEs ( = 0.03) and grade ≥ 3 TRAEs ( < 0.0001).
As for the efficacy and safety outcome, compared with standard chemotherapy, dual immunotherapy remains an effective first-line therapy for patients with advanced NSCLC, especially for patients with high TMB levels and squamous cell histology. Furthermore, compared to single-agent immunotherapy, dual immunotherapy is only considered for use in patients with low PD-L1 expression in order to reduce the emergence of resistance to immunotherapy. https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42022336614.
近期临床试验证实,抗程序性细胞死亡蛋白1/配体1(抗PD-1/L1)联合抗细胞毒性T淋巴细胞相关蛋白4(抗CTLA-4)或抗具有Ig和ITIM结构域的T细胞免疫受体(TIGIT)抗体(双重免疫疗法)作为晚期非小细胞肺癌(NSCLC)患者的一线治疗方案带来了显著益处。然而,其不良反应发生率也有所增加,不容忽视。本研究旨在探讨双重免疫疗法在晚期NSCLC中的疗效和安全性。
本荟萃分析最终纳入了截至2022年8月13日从PubMed、EMBASE和Cochrane对照试验中央注册库数据库收集的9项一线随机对照试验。疗效以无进展生存期(PFS)、总生存期(OS)的风险比(HR)和95%置信区间(CI)以及客观缓解率(ORR)的风险比(RR)来衡量。通过任何级别的治疗相关不良事件(TRAEs)和≥3级TRAEs的RR评估治疗安全性。
我们的结果表明,与化疗相比,双重免疫疗法在所有PD-L1表达水平的OS(HR = 0.76,95% CI:0.69 - 0.82)和PFS(HR = 0.75,95% CI:0.67 - 0.83)方面均显示出持久益处。亚组分析还表明,与化疗相比,双重免疫疗法使肿瘤突变负荷(TMB)高的患者(OS:HR = 0.76,P = 0.0009;PFS:HR = 0.72,P < 0.0001)和鳞状细胞组织学患者(OS:HR = 0.64,P < 0.00001;PFS:HR = 0.66,P < 0.001)的长期生存率得到改善。然而,与免疫检查点抑制剂(ICI)单药治疗相比,双重免疫疗法在OS和ORR方面显示出一些优势,且仅在PD-L1 < 25%时改善了PFS(HR = 0.77,P = 0.005)。在安全性方面,双重免疫疗法组与化疗组在任何级别的TRAEs(P = 0.05)和≥3级TRAEs(P = 0.31)上无显著差异。然而,与ICI单药治疗相比,双重免疫疗法显著增加了任何级别的TRAEs(P = 0.03)和≥3级TRAEs(P < 0.0001)的发生率。
就疗效和安全性结果而言,与标准化疗相比,双重免疫疗法仍然是晚期NSCLC患者有效的一线治疗方案,特别是对于TMB水平高和鳞状细胞组织学的患者。此外,与单药免疫疗法相比,双重免疫疗法仅考虑用于PD-L1表达低的患者,以减少免疫治疗耐药性的出现。https://www.crd.york.ac.uk/PROSPERO/,标识符CRD42022336614。