Department of Global Health.
Department of Epidemiology, University of Washington, Seattle, WA, USA.
J Infect Dis. 2024 Apr 12;229(4):988-998. doi: 10.1093/infdis/jiad252.
Bacterial pathogens cause substantial diarrhea morbidity and mortality among children living in endemic settings, yet antimicrobial treatment is only recommended for dysentery or suspected cholera.
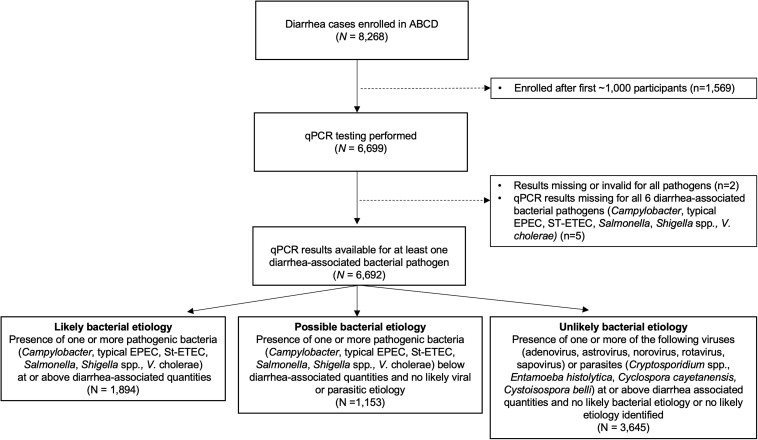
AntiBiotics for Children with severe Diarrhea was a 7-country, placebo-controlled, double-blind efficacy trial of azithromycin in children 2-23 months of age with watery diarrhea accompanied by dehydration or malnutrition. We tested fecal samples for enteric pathogens utilizing quantitative polymerase chain reaction to identify likely and possible bacterial etiologies and employed pathogen-specific cutoffs based on genomic target quantity in previous case-control diarrhea etiology studies to identify likely and possible bacterial etiologies.
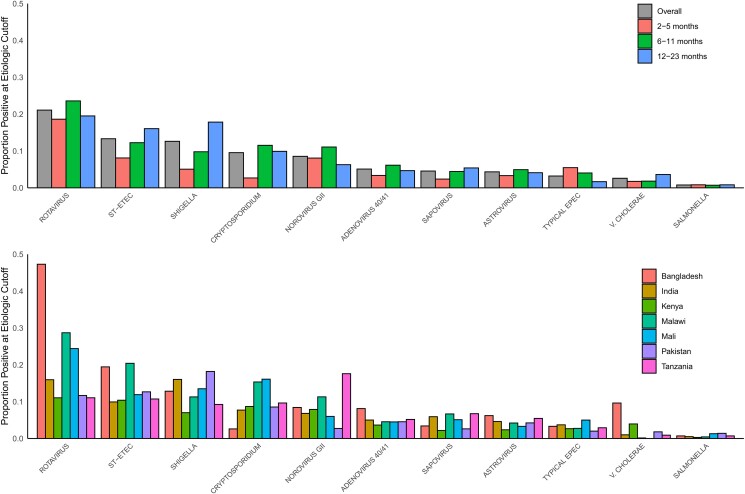
Among 6692 children, the leading likely etiologies were rotavirus (21.1%), enterotoxigenic Escherichia coli encoding heat-stable toxin (13.3%), Shigella (12.6%), and Cryptosporidium (9.6%). More than one-quarter (1894 [28.3%]) had a likely and 1153 (17.3%) a possible bacterial etiology. Day 3 diarrhea was less common in those randomized to azithromycin versus placebo among children with a likely bacterial etiology (risk difference [RD]likely, -11.6 [95% confidence interval {CI}, -15.6 to -7.6]) and possible bacterial etiology (RDpossible, -8.7 [95% CI, -13.0 to -4.4]) but not in other children (RDunlikely, -0.3% [95% CI, -2.9% to 2.3%]). A similar association was observed for 90-day hospitalization or death (RDlikely, -3.1 [95% CI, -5.3 to -1.0]; RDpossible, -2.3 [95% CI, -4.5 to -.01]; RDunlikely, -0.6 [95% CI, -1.9 to .6]). The magnitude of risk differences was similar among specific likely bacterial etiologies, including Shigella.
Acute watery diarrhea confirmed or presumed to be of bacterial etiology may benefit from azithromycin treatment.
NCT03130114.
在流行地区生活的儿童中,细菌病原体可导致大量腹泻发病和死亡,但仅建议对痢疾或疑似霍乱使用抗菌药物治疗。
严重腹泻儿童使用阿奇霉素(AntiBiotics for Children with severe Diarrhea)是一项在 7 个国家开展的、安慰剂对照、双盲的阿奇霉素疗效试验,纳入年龄为 2-23 个月、伴有脱水或营养不良的水样腹泻儿童。我们利用定量聚合酶链反应检测粪便样本中的肠道病原体,以确定可能和确定的细菌病因,并根据以前的病例对照腹泻病因研究中基于基因组靶标数量的病原体特异性截止值来确定可能和确定的细菌病因。
在 6692 名儿童中,主要的可能病因是轮状病毒(21.1%)、编码热稳定毒素的肠毒性大肠杆菌(13.3%)、志贺菌(12.6%)和隐孢子虫(9.6%)。超过四分之一(1894 [28.3%])的儿童存在可能的细菌病因,1153 名(17.3%)存在可能的细菌病因。在有确定细菌病因的儿童中,与安慰剂相比,阿奇霉素治疗组第 3 天腹泻较少(可能病因的风险差异[RD],-11.6 [95%置信区间{CI},-15.6 至-7.6];可能病因的风险差异[RD],-8.7 [95% CI,-13.0 至-4.4]),但在其他儿童中未见差异(不太可能病因的风险差异[RD],-0.3% [95% CI,-2.9% 至 2.3%])。同样的关联也见于 90 天住院或死亡(可能病因的风险差异[RD],-3.1 [95% CI,-5.3 至-1.0];可能病因的风险差异[RD],-2.3 [95% CI,-4.5 至-.01];不太可能病因的风险差异[RD],-0.6 [95% CI,-1.9 至.6])。在特定的确定细菌病因中,阿奇霉素治疗的风险差异幅度相似,包括志贺菌。
急性水样腹泻确诊或推测为细菌病因时,可能受益于阿奇霉素治疗。
NCT03130114。