Department of Thoracic/Head and Neck Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
Department of Obstetrics and Gynecology, Shanghai General Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, China.
Front Immunol. 2023 Jun 28;14:1161869. doi: 10.3389/fimmu.2023.1161869. eCollection 2023.
Despite significant clinical advancement with the use of immune checkpoint blockade (ICB) in non-small cell lung cancer (NSCLC) there are still a major subset of patients that develop adaptive/acquired resistance. Understanding resistance mechanisms to ICB is critical to developing new therapeutic strategies and improving patient survival. The dynamic nature of the tumor microenvironment and the mutational load driving tumor immunogenicity limit the efficacy to ICB. Recent studies indicate that myeloid cells are drivers of ICB resistance. In this study we sought to understand which immune cells were contributing to resistance and if we could modify them in a way to improve response to ICB therapy.
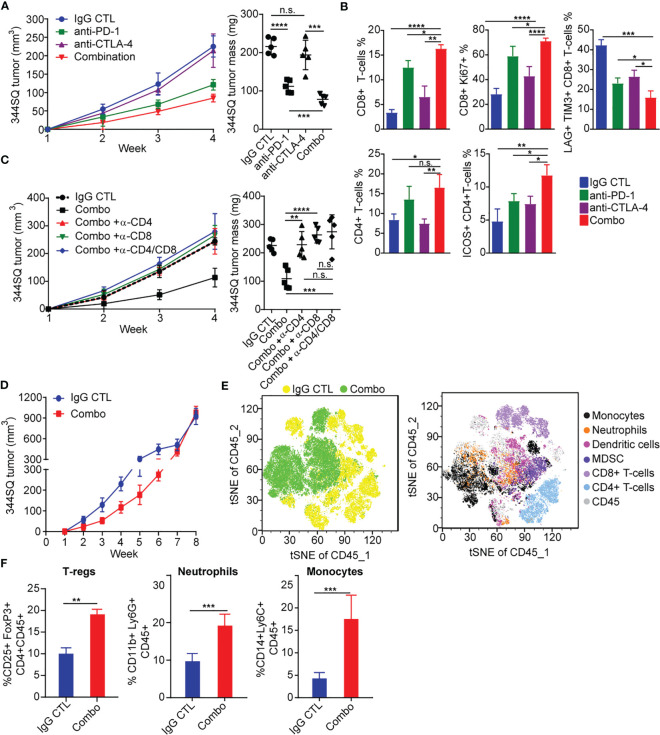
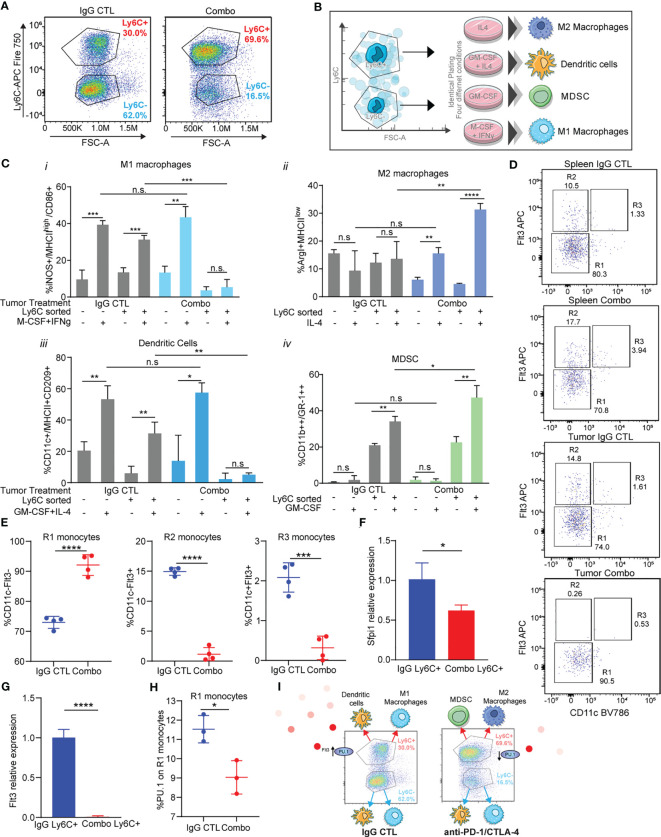
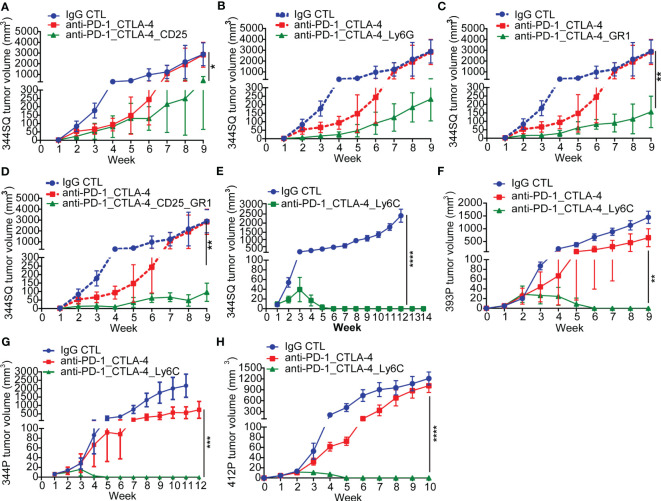
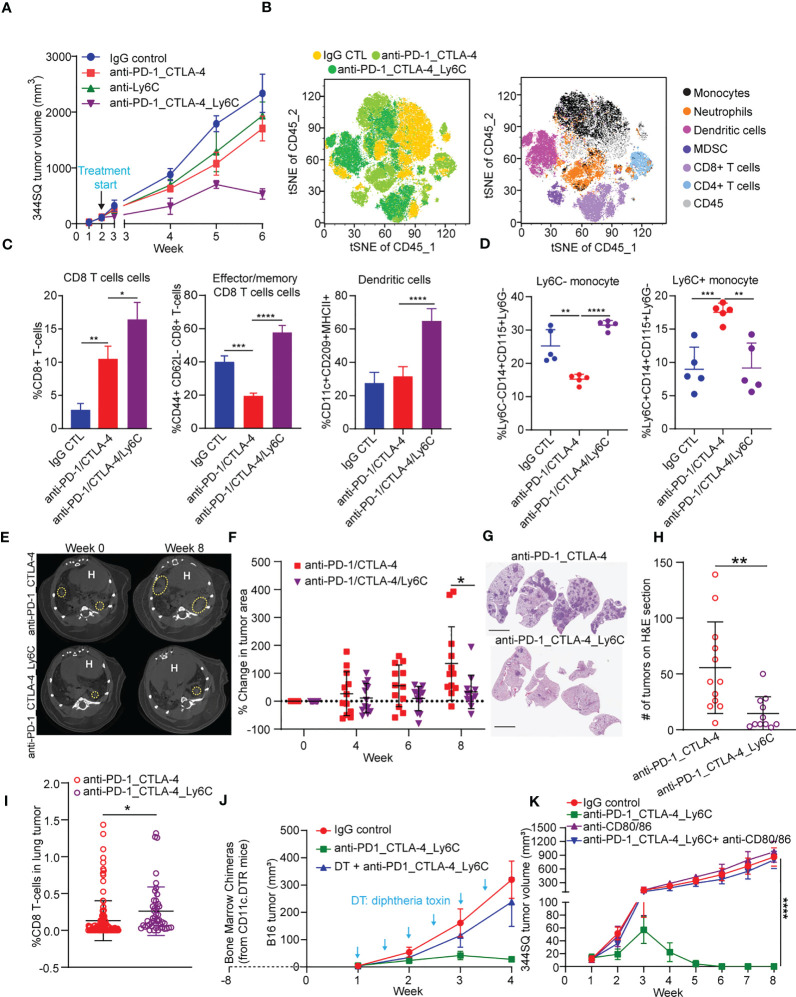
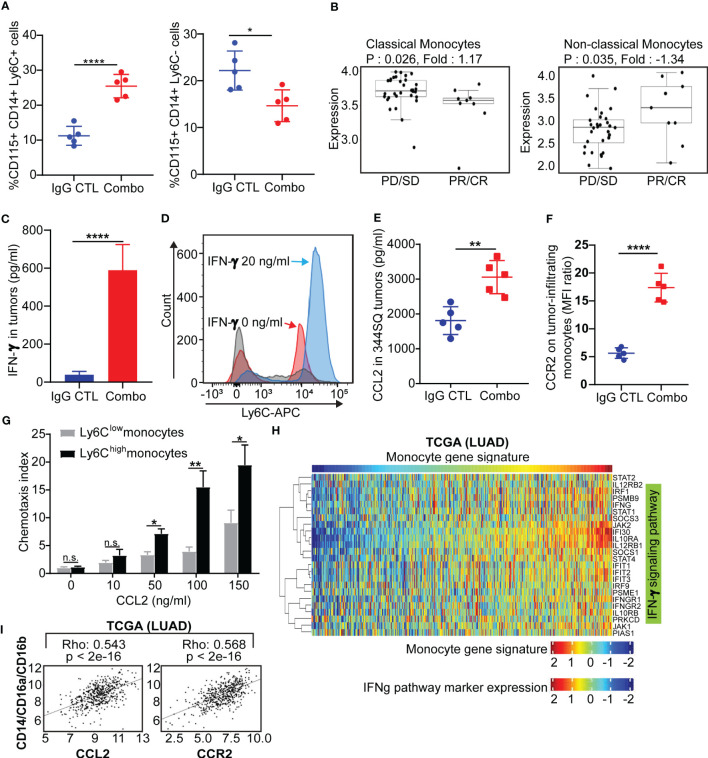
Our results show that combination anti-PD-1/CTLA-4 produces an initial antitumor effect with evidence of an activated immune response. Upon extended treatment with anti-PD-1/CTLA-4 acquired resistance developed with an increase of the immunosuppressive populations, including T-regulatory cells, neutrophils and monocytes. Addition of anti-Ly6C blocking antibody to anti-PD-1/CTLA-4 was capable of completely reversing treatment resistance and restoring CD8 T cell activity in multiple KP lung cancer models and in the autochthonous lung cancer Kras/p53 model. We found that there were higher classical Ly6C+ monocytes in anti-PD-1/CTLA-4 combination resistant tumors. B7 blockade illustrated the importance of dendritic cells for treatment efficacy of anti-Ly6C/PD-1/CTLA-4. We further determined that classical Ly6C+ monocytes in anti-PD-1/CTLA-4 resistant tumors are trafficked into the tumor via IFN-γ and the CCL2-CCR2 axis. Mechanistically we found that classical monocytes from ICB resistant tumors were unable to differentiate into antigen presenting cells and instead differentiated into immunosuppressive M2 macrophages or myeloid-derived suppressor cells (MDSC). Classical Ly6C+ monocytes from ICB resistant tumors had a decrease in both Flt3 and PU.1 expression that prevented differentiation into dendritic cells/macrophages.
Therapeutically we found that addition of anti-Ly6C to the combination of anti-PD-1/CTLA-4 was capable of complete tumor eradication. Classical Ly6C+ monocytes differentiate into immunosuppressive cells, while blockade of classical monocytes drives dendritic cell differentiation/maturation to reinvigorate the anti-tumor T cell response. These findings support that immunotherapy resistance is associated with infiltrating monocytes and that controlling the differentiation process of monocytes can enhance the therapeutic potential of ICB.
尽管在非小细胞肺癌 (NSCLC) 中使用免疫检查点阻断 (ICB) 取得了重大临床进展,但仍有相当一部分患者出现适应性/获得性耐药。了解对 ICB 的耐药机制对于开发新的治疗策略和提高患者生存率至关重要。肿瘤微环境的动态性质和驱动肿瘤免疫原性的突变负荷限制了 ICB 的疗效。最近的研究表明,髓样细胞是 ICB 耐药的驱动因素。在这项研究中,我们试图了解哪些免疫细胞有助于耐药,并确定是否可以通过改变它们来提高对 ICB 治疗的反应。
我们的结果表明,联合使用抗 PD-1/CTLA-4 可产生初始抗肿瘤作用,并证明存在激活的免疫反应。在延长抗 PD-1/CTLA-4 治疗后,出现了获得性耐药,免疫抑制群体(包括 T 调节细胞、中性粒细胞和单核细胞)增加。在多个 KP 肺癌模型和自发肺肿瘤 Kras/p53 模型中,抗 PD-1/CTLA-4 中添加抗 Ly6C 阻断抗体能够完全逆转治疗耐药并恢复 CD8 T 细胞活性。我们发现,在抗 PD-1/CTLA-4 联合耐药肿瘤中存在更高水平的经典 Ly6C+单核细胞。B7 阻断表明树突状细胞对抗 Ly6C/PD-1/CTLA-4 的治疗效果很重要。我们进一步确定,在抗 PD-1/CTLA-4 耐药肿瘤中,经典 Ly6C+单核细胞通过 IFN-γ 和 CCL2-CCR2 轴被运送到肿瘤中。从机制上讲,我们发现来自 ICB 耐药肿瘤的经典单核细胞无法分化为抗原呈递细胞,而是分化为免疫抑制性 M2 巨噬细胞或髓源性抑制细胞 (MDSC)。来自 ICB 耐药肿瘤的经典 Ly6C+单核细胞的 Flt3 和 PU.1 表达减少,阻止了其向树突状细胞/巨噬细胞分化。
在治疗方面,我们发现抗 Ly6C 与抗 PD-1/CTLA-4 联合使用可完全消除肿瘤。经典 Ly6C+单核细胞分化为免疫抑制细胞,而阻断经典单核细胞可驱动树突状细胞分化/成熟,从而重新激活抗肿瘤 T 细胞反应。这些发现支持免疫治疗耐药与浸润单核细胞有关,并且控制单核细胞的分化过程可以增强 ICB 的治疗潜力。