Oncology Department, The Third People's Hospital of Hubei Province, Affiliated Hospital of Jianghan University, 26# Zhongshan Avenue, Qiaokou District, Wuhan, 430033, Hubei Province, China.
Sci Rep. 2023 Jul 26;13(1):12071. doi: 10.1038/s41598-023-39211-5.
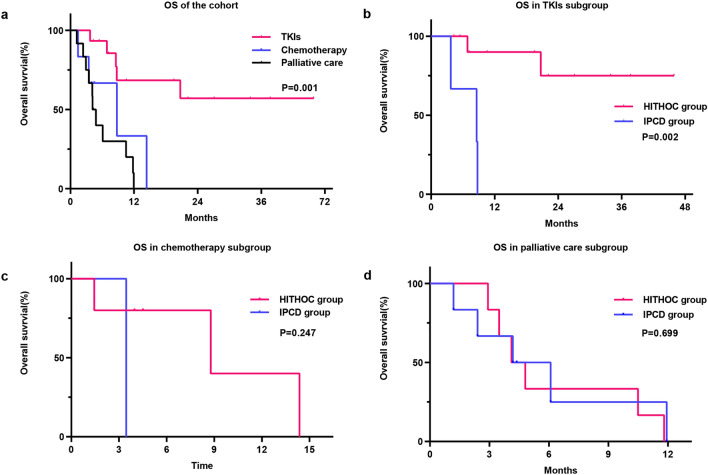
Initially diagnosed malignant pleural effusion (MPE) has different systematic treatments, and defining the best drainage regimen according to the responsiveness of MPE to different systematic treatments is important. This study compared the efficacy of hyperthermic intrathoracic chemotherapy (HITHOC) and pleural catheter drainage (IPCD) for initially diagnosed lung cancer with symptomatic MPE. We retrospectively reviewed the medical records of initially diagnosed lung cancer patients with symptomatic MPE between January 2018 and May 2022. The patients were treated with IPCD or HITHOC for local control of MPE after diagnosis. Systematic regimens were conducted during 1 month according to guidelines after local treatment. Intrathoracic MPE progression-free survival (iPFS) and overall survival (OS) were calculated, Univariate and multivariable Cox-regression were used to identify factors associated with iPFS and OS. A total of 33 patients were evaluated; 10 (30.3%) patients received IPCD, and 23 (69.7%) patients received HITHOC. No difference in the MPE control rate at 1 month was found between the IPCD group (90%) and HITHOC group (95.7%). However, this control rate was significantly higher in the HITHOC group (69.6%) than in the IPCD group (30%) at 3 months (P = 0.035). Multivariate analysis showed that receiving tyrosine kinase inhibitors (TKIs) or chemotherapy was a significant protective factor for iPFS (HR = 0.376, 95% CI 0.214-0.659, P = 0.007) and OS (HR = 0.321, 95% CI 0.174-0.594, P < 0.001). According to subgroup analysis, among patients treated with TKIs, those who received HITHOC had longer iPFS and OS than those who received IPCD (P = 0.011 and P = 0.002, respectively), but this difference was not found in the palliative care subgroup. Moreover, no patients treated with chemotherapy showed reaccumulation of MPE. Systematic TKIs or chemotherapy prolonged iPFS and OS for those initially diagnosed with lung cancer with symptomatic MPE. HITHOC prolonged iPFS and OS for those treated with systematic TKIs.
最初诊断为恶性胸腔积液 (MPE) 有不同的系统治疗方法,根据 MPE 对不同系统治疗的反应来确定最佳引流方案非常重要。本研究比较了高热胸腔内化疗 (HITHOC) 和胸腔导管引流 (IPCD) 对有症状的 MPE 的初始诊断肺癌的疗效。我们回顾性分析了 2018 年 1 月至 2022 年 5 月间初诊肺癌合并有症状 MPE 患者的病历。患者在诊断后采用 IPCD 或 HITHOC 进行 MPE 的局部控制。局部治疗后,根据指南进行 1 个月的系统治疗。计算胸腔内 MPE 无进展生存期 (iPFS) 和总生存期 (OS)。采用单变量和多变量 Cox 回归分析确定与 iPFS 和 OS 相关的因素。共评估了 33 例患者;10 例 (30.3%)患者接受 IPCD,23 例 (69.7%)患者接受 HITHOC。1 个月时 IPCD 组 (90%)与 HITHOC 组 (95.7%)的 MPE 控制率无差异。然而,3 个月时 HITHOC 组 (69.6%)的控制率明显高于 IPCD 组 (30%) (P = 0.035)。多变量分析显示,接受酪氨酸激酶抑制剂 (TKI) 或化疗是 iPFS (HR = 0.376, 95% CI 0.214-0.659, P = 0.007) 和 OS (HR = 0.321, 95% CI 0.174-0.594, P < 0.001) 的显著保护因素。根据亚组分析,在接受 TKI 治疗的患者中,接受 HITHOC 治疗的患者 iPFS 和 OS 长于接受 IPCD 治疗的患者 (P = 0.011 和 P = 0.002),但在姑息治疗亚组中未发现这种差异。此外,接受化疗的患者均未出现 MPE 再积聚。系统 TKI 或化疗延长了有症状的 MPE 的初诊肺癌患者的 iPFS 和 OS。HITHOC 延长了接受系统 TKI 治疗的患者的 iPFS 和 OS。