Deng Hansen, Puccio David J, Anand Sharath K, Yue John K, Hudson Joseph S, Legarreta Andrew D, Wei Zhishuo, Okonkwo David O, Puccio Ava M, Nwachuku Enyinna L
Department of Neurological Surgery, University of Pittsburgh Medical Center, 200 Lothrop Street, Suite B-400, Pittsburgh, PA 15213, USA.
Department of Neurological Surgery, University of California San Francisco, San Francisco, CA 94110, USA.
Diagnostics (Basel). 2023 Jul 21;13(14):2434. doi: 10.3390/diagnostics13142434.
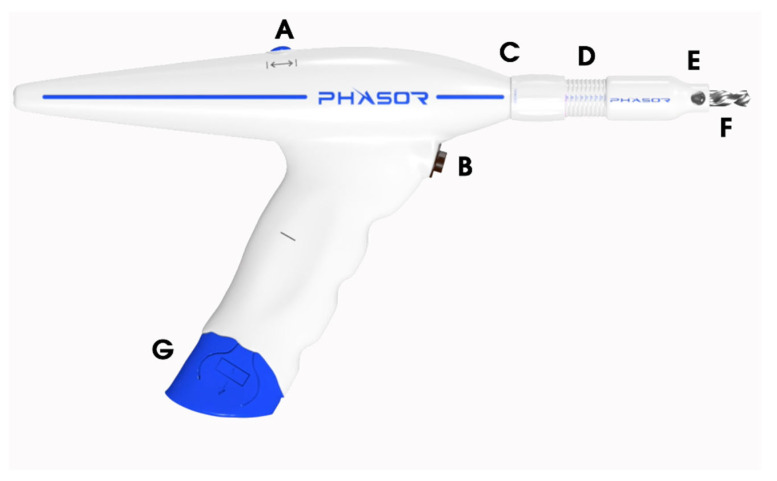
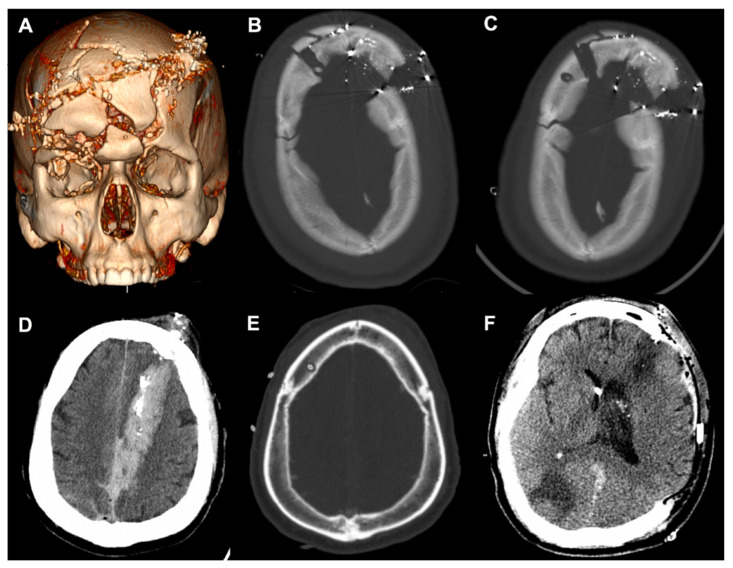
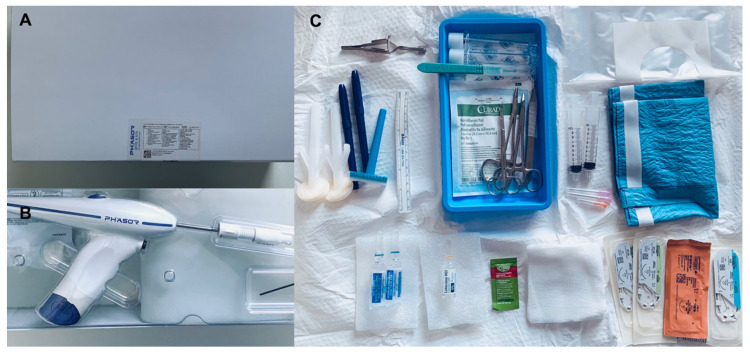
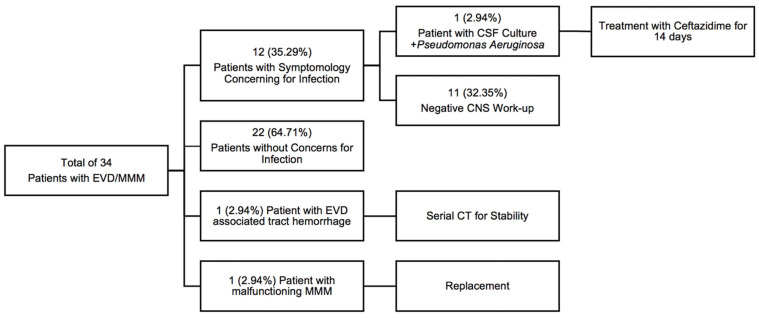
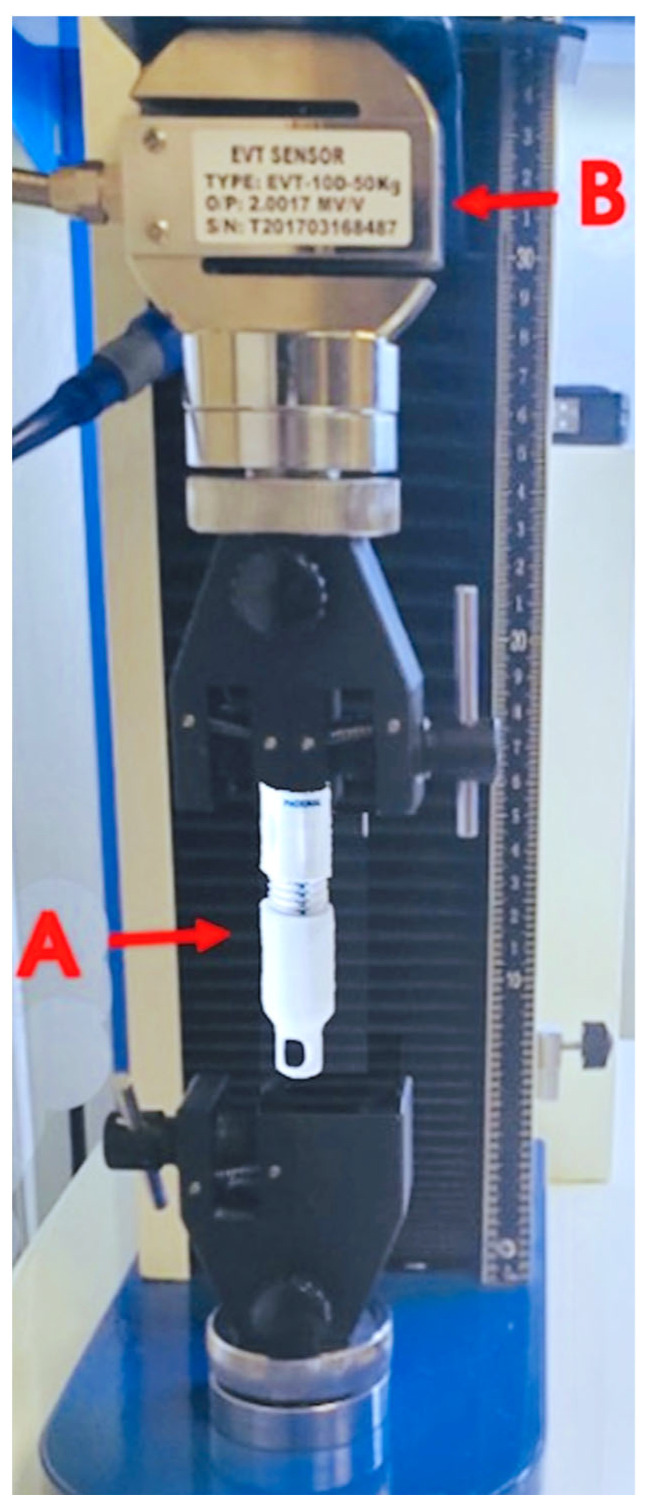
Invasive neuromonitoring is a bedrock procedure in neurosurgery and neurocritical care. Intracranial hypertension is a recognized emergency that can potentially lead to herniation, ischemia, and neurological decline. Over 50,000 external ventricular drains (EVDs) are performed in the United States annually for traumatic brain injuries (TBI), tumors, cerebrovascular hemorrhaging, and other causes. The technical challenge of a bedside ventriculostomy and/or parenchymal monitor placement may be increased by complex craniofacial trauma or brain swelling, which will decrease the tolerance of brain parenchyma to applied procedural force during a craniostomy. Herein, we report on the implementation and safety of a disposable power drill for bedside neurosurgical practices compared with the manual twist drill that is the current gold standard. Mechanical testing of the drill's stop extension (n = 8) was conducted through a calibrated tensile tester, simulating an axial plunging of 22.68 kilogram (kg) or 50 pounds of force (lbf) and measuring the strength-responsive displacement. The mean displacement following compression was 0.18 ± 0.11 mm (range of 0.03 mm to 0.34 mm). An overall cost analysis was calculated based on the annual institutional pricing, with an estimated $64.90 per unit increase in the cost of the disposable electric drill. Power drill craniostomies were utilized in a total of 34 adult patients, with a median Glasgow Coma Scale (GCS) score of six. Twenty-seven patients were male, with a mean age of 50.7 years old. The two most common injury mechanisms were falls and motor vehicle/motorcycle accidents. EVDs were placed in all subjects, and additional quad-lumen neuromonitoring was applied to 23 patients, with no incidents of plunging events or malfunctions. One patient developed an intracranial infection and another had intraparenchymal tract hemorrhaging. Two illustrative TBI cases with concomitant craniofacial trauma were provided. The disposable power drill was successfully implemented as an option for bedside ventriculostomies and had an acceptable safety profile.
有创神经监测是神经外科和神经重症监护中的一项基础操作。颅内高压是一种公认的急症,可能导致脑疝、缺血和神经功能衰退。在美国,每年有超过50000例因创伤性脑损伤(TBI)、肿瘤、脑血管出血及其他原因而进行的体外脑室引流(EVD)操作。复杂的颅面创伤或脑肿胀可能会增加床边脑室造瘘术和/或实质监测器放置的技术难度,这会降低开颅手术期间脑实质对施加的手术力的耐受性。在此,我们报告一种一次性电钻在床边神经外科手术中的应用及安全性,并与作为当前金标准的手动麻花钻进行比较。通过校准拉伸试验机对该电钻的止动延伸装置进行了机械测试(n = 8),模拟22.68千克(kg)或50磅力(lbf)的轴向插入,并测量强度响应位移。压缩后的平均位移为0.18±0.11毫米(范围为0.03毫米至0.34毫米)。基于机构年度定价进行了总体成本分析,估计一次性电钻的成本每单位增加64.90美元。总共34例成年患者使用了电钻开颅术,格拉斯哥昏迷量表(GCS)评分中位数为6分。27例患者为男性,平均年龄为50.7岁。两种最常见的损伤机制是跌倒和机动车/摩托车事故。所有受试者均放置了EVD,另外23例患者应用了四腔神经监测,未发生插入事件或故障。1例患者发生颅内感染,另1例出现脑实质内通道出血。提供了2例伴有颅面创伤的典型TBI病例。一次性电钻作为床边脑室造瘘术的一种选择已成功实施,且具有可接受的安全性。