Mantovani Alessandro, Herbort Carl P, Hedayatfar Alireza, Papasavvas Ioannis
Department of Ophthalmology, Valduce Hospital, 22100 Como, Italy.
Inflammatory and Retinal Eye Diseases, Centre for Ophthalmic Specialised Care (COS), 1003 Lausanne, Switzerland.
Diagnostics (Basel). 2023 Jul 24;13(14):2466. doi: 10.3390/diagnostics13142466.
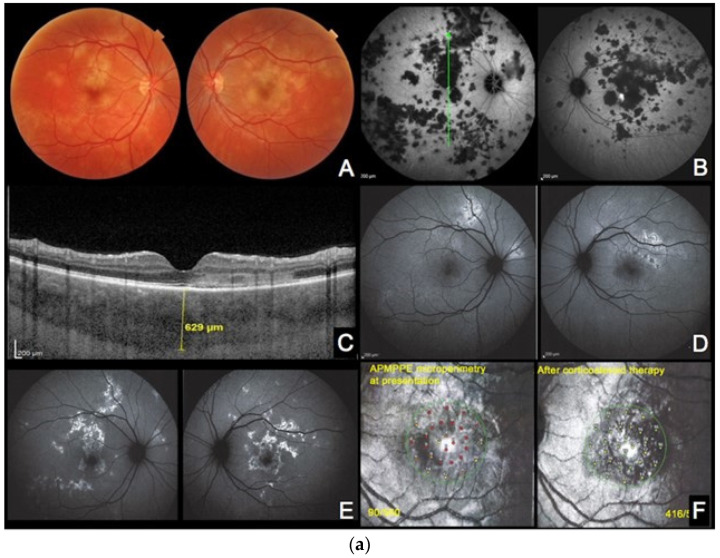
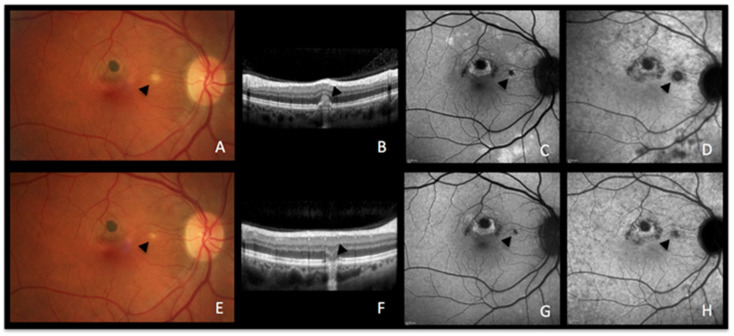
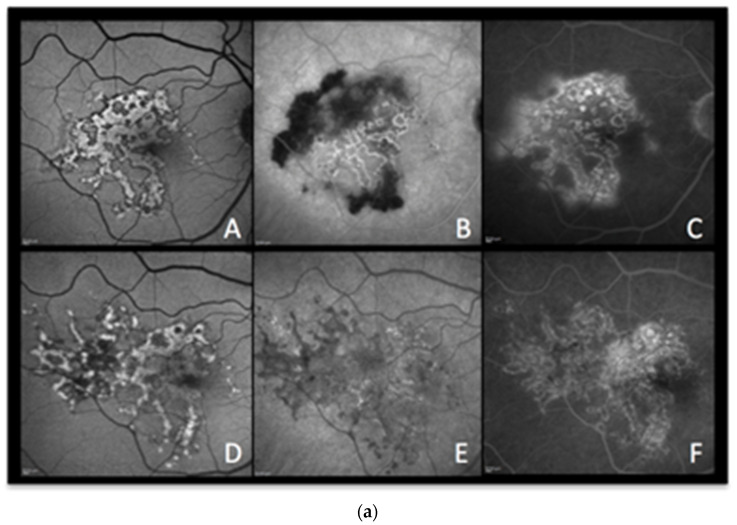
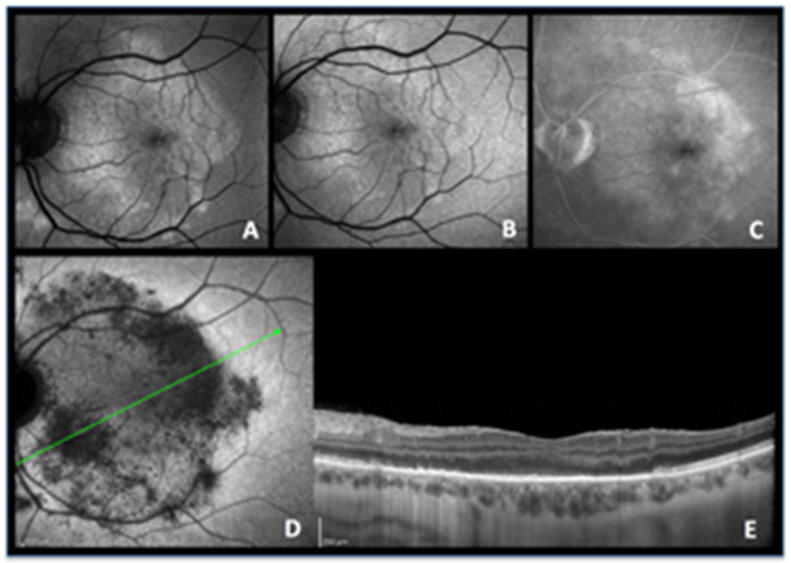
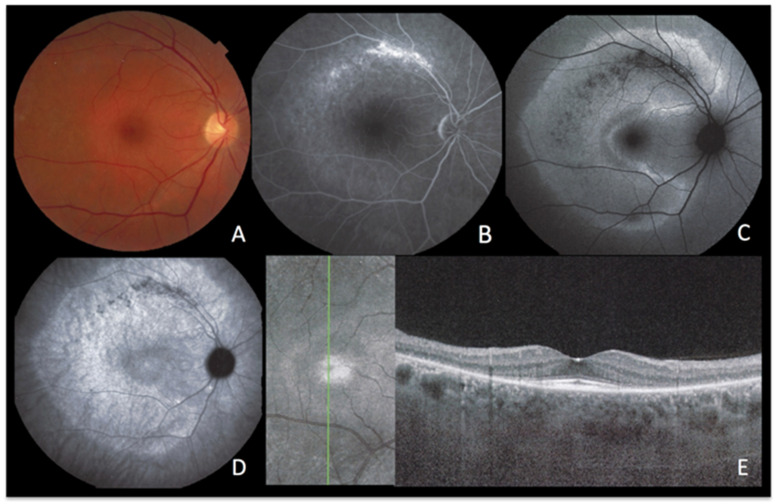
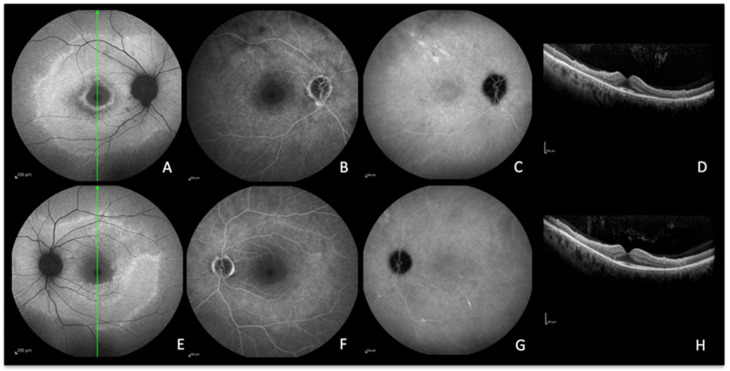
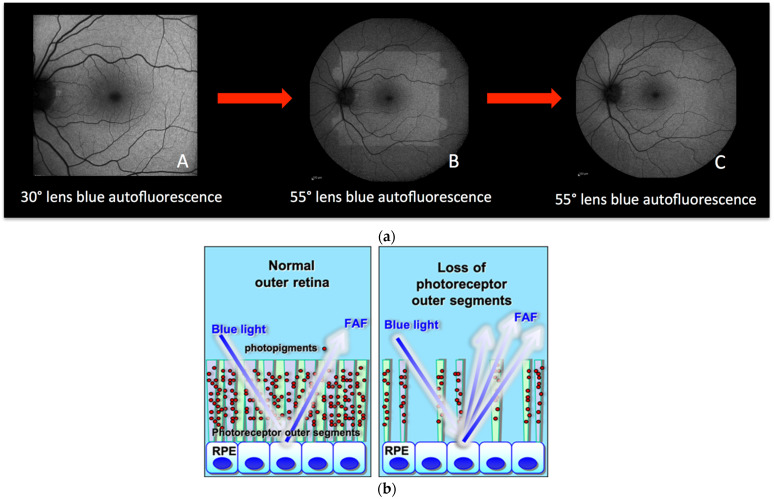
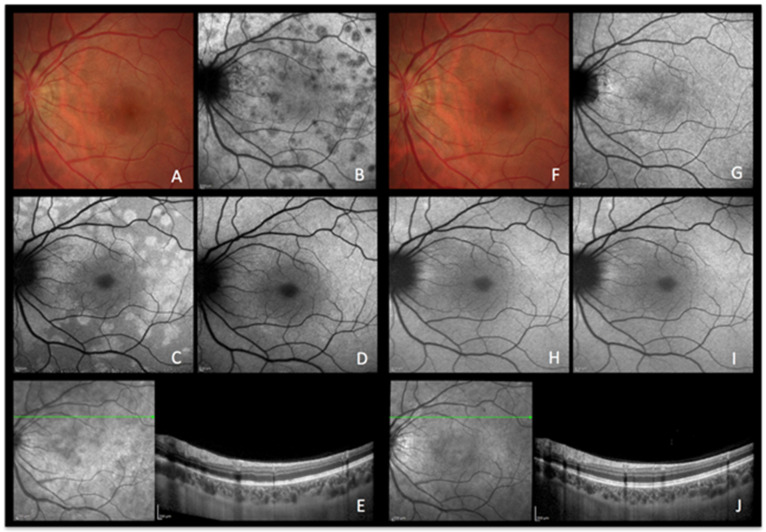
Our purpose is to describe blue-light fundus autofluorescence (BAF) features of inflammatory diseases of the outer retina characterised by photoreceptor damage. BAF from patients diagnosed with secondary and primary inflammatory photoreceptor damage were retrospectively analyzed and compared to other imaging modalities including fluorescein angiography (FA), indocyanine green angiography (ICGA), and spectral domain optical coherence tomography (SD-OCT). Multiple evanescent white dot syndrome (MEWDS), idiopathic multifocal choroiditis (MFC), acute posterior multifocal placoid pigment epitheliopathy (APMPPE), serpiginous choroiditis (SC), and acute syphilitic posterior placoid chorioretinitis (ASPPC), all cases corresponding to secondary photoreceptor diseases caused by inflammatory choriocapillaris nonperfusion, were included and compared to primary photoreceptor disease entities, including acute zonal occult outer retinopathy (AZOOR) and cancer-associated retinopathy (CAR). Both groups showed increased BAFs of variable intensity. In severe cases of APMPPE and ASPPC, BAF also showed hypoautofluorescent areas. In group 1 (secondary diseases) BAF hyperautofluorescent areas were associated with colocalized ICGA hypofluorescent areas, indicating choriocapillaris nonperfusion; whereas in group 2 (primary diseases), no ICGA signs were detected. The associated colocalized areas of hypofluorescence on ICGA in the first group, which were absent in the second group, were crucial to allow the differentiation between primary (photoreceptoritis) and secondary (choriocapillaritis) photoreceptor diseases. BAF patterns in inflammatory diseases of the outer retina can give relevant information on the photoreceptor and RPE involvement, with ICGA being crucial to detect concurring choriocapillaris damage and differentiating the two pathologies.
我们的目的是描述以光感受器损伤为特征的外层视网膜炎症性疾病的蓝光眼底自发荧光(BAF)特征。对诊断为继发性和原发性炎症性光感受器损伤患者的BAF进行回顾性分析,并与其他成像方式进行比较,包括荧光素血管造影(FA)、吲哚菁绿血管造影(ICGA)和光谱域光学相干断层扫描(SD-OCT)。纳入了多发性瞬目白点综合征(MEWDS)、特发性多灶性脉络膜炎(MFC)、急性后极部多灶性鳞状色素上皮病变(APMPPE)、匐行性脉络膜炎(SC)和急性梅毒性后极部鳞状脉络膜视网膜炎(ASPPC),所有病例均对应于由炎症性脉络膜毛细血管无灌注引起的继发性光感受器疾病,并与原发性光感受器疾病实体进行比较,包括急性区域性隐匿性外层视网膜病变(AZOOR)和癌症相关性视网膜病变(CAR)。两组均显示出不同强度的BAF增加。在APMPPE和ASPPC的严重病例中,BAF也显示出自发荧光减低区域。在第1组(继发性疾病)中,BAF高自发荧光区域与ICGA低荧光区域共定位,表明脉络膜毛细血管无灌注;而在第2组(原发性疾病)中,未检测到ICGA征象。第一组ICGA上相关的低荧光共定位区域在第二组中不存在,这对于区分原发性(光感受器炎)和继发性(脉络膜毛细血管炎)光感受器疾病至关重要。外层视网膜炎症性疾病中的BAF模式可以提供有关光感受器和视网膜色素上皮受累的相关信息,ICGA对于检测并发的脉络膜毛细血管损伤和区分这两种病理情况至关重要。