Department of Surgery, Georgetown University Medical School, Washington, DC 20007, USA.
Department of Pediatrics, MedStar Georgetown University Hospital, Washington, DC 20007, USA.
Viruses. 2023 Jul 16;15(7):1559. doi: 10.3390/v15071559.
Planning for future resurgences in SARS-CoV-2 infection is necessary for providers who care for immunocompromised patients.
to determine factors associated with COVID-19 disease severity in immunosuppressed children.
a case series of children with solid organ transplants diagnosed with SARS-CoV-2 infection between 15 March 2020 and 31 March 2023.
a single pediatric transplant center.
all children with a composite transplant (liver, pancreas, intestine), isolated intestine transplant (IT), isolated liver transplant LT), or simultaneous liver kidney transplant (SLK) with a positive PCR for SARS-CoV-2.
SARS-CoV-2 infection.
We hypothesized that children on the most immunosuppression, defined by the number of immunosuppressive medications and usage of steroids, would have the most severe disease course and that differential white blood cell count in the months preceding infection would be associated with likelihood of having severe disease. The hypothesis being tested was formulated during data collection. The primary study outcome measurement was disease severity defined using WHO criteria.
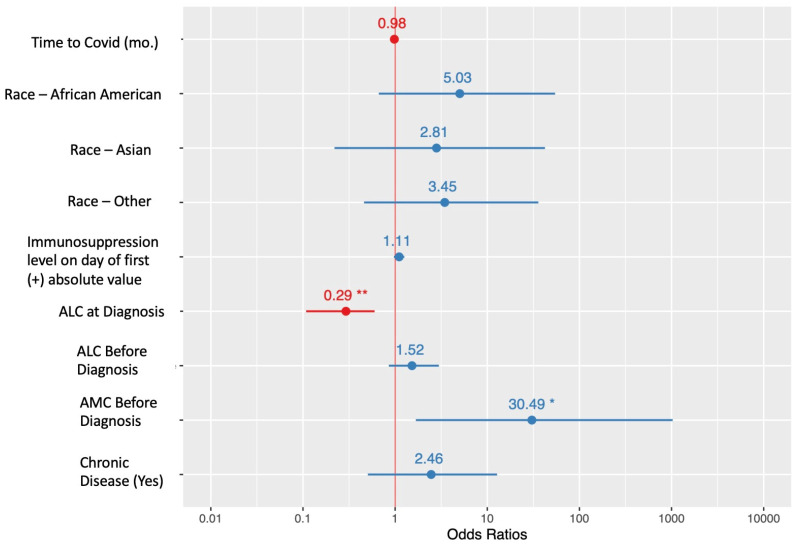
77 children (50 LT, 24 intestine, 3 SLK) were infected with SARS-CoV-2, 57.4 months from transplant (IQR 19.7-87.2). 17% were ≤1 year post transplant at infection. 55% were male, 58% were symptomatic and ~29% had severe disease. A high absolute lymphocyte count at diagnosis decreased the odds of having severe COVID-19 disease (OR 0.29; CI 0.11-0.60; = 0.004). Conversely, patients with a high absolute monocyte count in the three months preceding infection had increased odds of having severe disease (OR 30.49; CI 1.68-1027.77; = 0.033). Steroid use, higher tacrolimus level, and number of immunosuppressive medications at infection did not increase the odds of having severe disease.
The significance of a high monocyte count as predictor of severe disease potentially confirms the importance of monocytic inflammasome-driven inflammation in COVID-19 pathogenesis. Our data do not support reducing immunosuppression in the setting of infection. Our observations may have important ramifications in resource management as vaccine- and infection-induced immunity wanes.
对于照顾免疫功能低下患者的医护人员来说,规划未来 SARS-CoV-2 感染的反弹是必要的。
确定与免疫抑制儿童 COVID-19 疾病严重程度相关的因素。
对 2020 年 3 月 15 日至 2023 年 3 月 31 日期间诊断为 SARS-CoV-2 感染的实体器官移植儿童的病例系列研究。
一家儿科移植中心。
所有接受复合移植(肝、胰腺、肠)、孤立性肠移植(IT)、孤立性肝移植(LT)或同时肝肾移植(SLK)的儿童,以及 SARS-CoV-2 阳性 PCR 的儿童。
SARS-CoV-2 感染。
我们假设,根据免疫抑制药物的数量和类固醇的使用情况,处于免疫抑制最强的儿童,疾病进展最严重,且在感染前几个月的白细胞计数差异与发生严重疾病的可能性相关。在数据收集过程中制定了正在测试的假设。主要研究结果的衡量标准是根据世界卫生组织(WHO)标准定义的疾病严重程度。
77 名儿童(50 名 LT、24 名肠、3 名 SLK)感染了 SARS-CoV-2,移植后 57.4 个月(IQR 19.7-87.2)。17%的儿童在感染时≤1 岁。55%为男性,58%有症状,约 29%的儿童患有严重疾病。诊断时高绝对值淋巴细胞计数降低了发生严重 COVID-19 疾病的几率(OR 0.29;CI 0.11-0.60; = 0.004)。相反,在感染前三个月中,高绝对值单核细胞计数的患者发生严重疾病的几率增加(OR 30.49;CI 1.68-1027.77; = 0.033)。感染时使用类固醇、更高的他克莫司水平和免疫抑制药物的数量并未增加发生严重疾病的几率。
单核细胞计数升高作为严重疾病预测指标的意义可能证实了单核细胞炎症小体驱动的炎症在 COVID-19 发病机制中的重要性。我们的数据不支持在感染时减少免疫抑制。我们的观察结果可能对资源管理具有重要意义,因为疫苗和感染诱导的免疫会减弱。