Cardiovascular Section, Department of Internal Medicine, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC, 27157, USA.
Quantitative Sciences Unit, Department of Medicine, Stanford University, Palo Alto, CA, USA.
Sci Rep. 2023 Jul 29;13(1):12290. doi: 10.1038/s41598-023-38782-7.
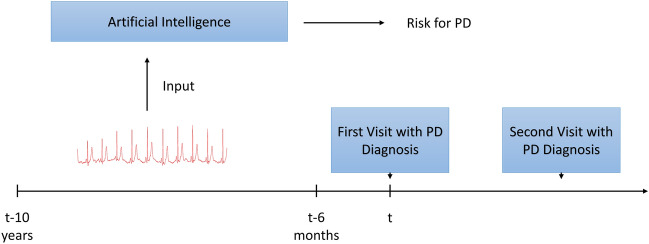
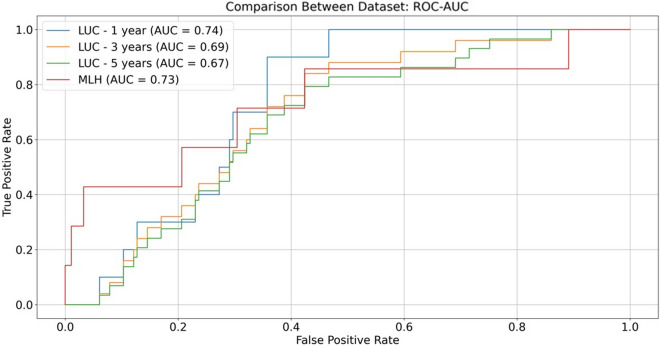
Little is known about electrocardiogram (ECG) markers of Parkinson's disease (PD) during the prodromal stage. The aim of the study was to build a generalizable ECG-based fully automatic artificial intelligence (AI) model to predict PD risk during the prodromal stage, up to 5 years before disease diagnosis. This case-control study included samples from Loyola University Chicago (LUC) and University of Tennessee-Methodist Le Bonheur Healthcare (MLH). Cases and controls were matched according to specific characteristics (date, age, sex and race). Clinical data were available from May, 2014 onward at LUC and from January, 2015 onward at MLH, while the ECG data were available as early as 1990 in both institutes. PD was denoted by at least two primary diagnostic codes (ICD9 332.0; ICD10 G20) at least 30 days apart. PD incidence date was defined as the earliest of first PD diagnostic code or PD-related medication prescription. ECGs obtained at least 6 months before PD incidence date were modeled to predict a subsequent diagnosis of PD within three time windows: 6 months-1 year, 6 months-3 years, and 6 months-5 years. We applied a novel deep neural network using standard 10-s 12-lead ECGs to predict PD risk at the prodromal phase. This model was compared to multiple feature engineering-based models. Subgroup analyses for sex, race and age were also performed. Our primary prediction model was a one-dimensional convolutional neural network (1D-CNN) that was built using 131 cases and 1058 controls from MLH, and externally validated on 29 cases and 165 controls from LUC. The model was trained on 90% of the MLH data, internally validated on the remaining 10% and externally validated on LUC data. The best performing model resulted in an external validation AUC of 0.67 when predicting future PD at any time between 6 months and 5 years after the ECG. Accuracy increased when restricted to ECGs obtained within 6 months to 3 years before PD diagnosis (AUC 0.69) and was highest when predicting future PD within 6 months to 1 year (AUC 0.74). The 1D-CNN model based on raw ECG data outperformed multiple models built using more standard ECG feature engineering approaches. These results demonstrate that a predictive model developed in one cohort using only raw 10-s ECGs can effectively classify individuals with prodromal PD in an independent cohort, particularly closer to disease diagnosis. Standard ECGs may help identify individuals with prodromal PD for cost-effective population-level early detection and inclusion in disease-modifying therapeutic trials.
关于帕金森病(PD)在前驱期的心电图(ECG)标志物知之甚少。本研究的目的是建立一个可推广的基于心电图的全自动人工智能(AI)模型,以预测前驱期 PD 风险,最长可预测至疾病诊断前 5 年。这项病例对照研究包括来自芝加哥洛约拉大学(LUC)和田纳西大学孟菲斯卫理公会大学健康中心(MLH)的样本。病例和对照组根据特定特征(日期、年龄、性别和种族)进行匹配。LUC 可从 2014 年 5 月起获取临床数据,MLH 可从 2015 年 1 月起获取临床数据,而两个机构的 ECG 数据早在 1990 年就已获取。PD 至少由两个原发性诊断代码(ICD9 332.0;ICD10 G20)表示,间隔至少 30 天。PD 发病日期定义为首次 PD 诊断代码或 PD 相关药物处方的最早日期。在 PD 发病日期至少 6 个月前获得的 ECG 用于建模,以预测在三个时间窗口内随后诊断为 PD 的情况:6 个月-1 年、6 个月-3 年和 6 个月-5 年。我们应用了一种新的深度神经网络,使用标准的 10 秒 12 导联 ECG 来预测前驱期的 PD 风险。该模型与基于多种特征工程的模型进行了比较。还对性别、种族和年龄进行了亚组分析。我们的主要预测模型是一维卷积神经网络(1D-CNN),该模型使用来自 MLH 的 131 例病例和 1058 例对照进行构建,并在来自 LUC 的 29 例病例和 165 例对照上进行了外部验证。该模型在 MLH 数据的 90%上进行训练,在剩余的 10%上进行内部验证,并在 LUC 数据上进行外部验证。在从 ECG 后 6 个月至 5 年内的任何时间预测未来 PD 时,表现最佳的模型在外部验证中的 AUC 为 0.67。当限制为在 PD 诊断前 6 个月至 3 年内获得的 ECG 时,准确性会提高(AUC 为 0.69),当在 6 个月至 1 年内预测未来 PD 时,准确性最高(AUC 为 0.74)。基于原始 ECG 数据的 1D-CNN 模型优于使用更标准的 ECG 特征工程方法构建的多个模型。这些结果表明,在一个队列中使用仅包含原始 10 秒 ECG 的预测模型可以在独立队列中有效地对前驱期 PD 患者进行分类,特别是在更接近疾病诊断时。标准 ECG 可能有助于识别前驱期 PD 患者,以便在人群层面进行具有成本效益的早期检测,并纳入疾病修正治疗试验。