Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, Evanston, Illinois, USA.
Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, Illinois, USA.
Magn Reson Med. 2023 Dec;90(6):2510-2523. doi: 10.1002/mrm.29776. Epub 2023 Aug 1.
After epicardial cardiac implantable electronic devices are implanted in pediatric patients, they become ineligible to receive MRI exams due to an elevated risk of RF heating. We investigated whether simple modifications in the trajectories of epicardial leads could substantially and reliably reduce RF heating during MRI at 1.5 T, with benefits extending to abandoned leads.
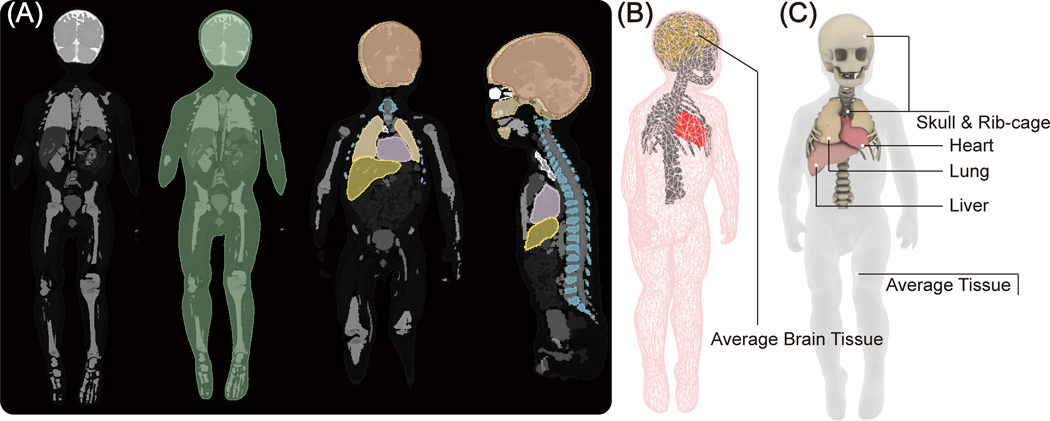
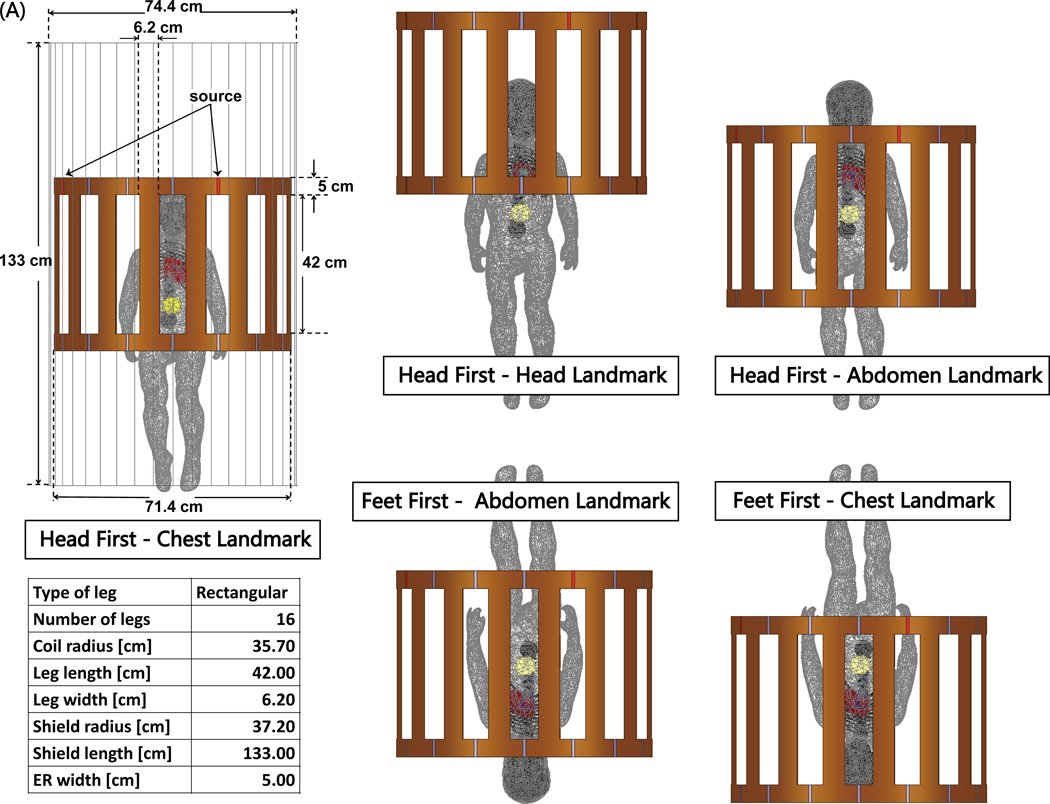
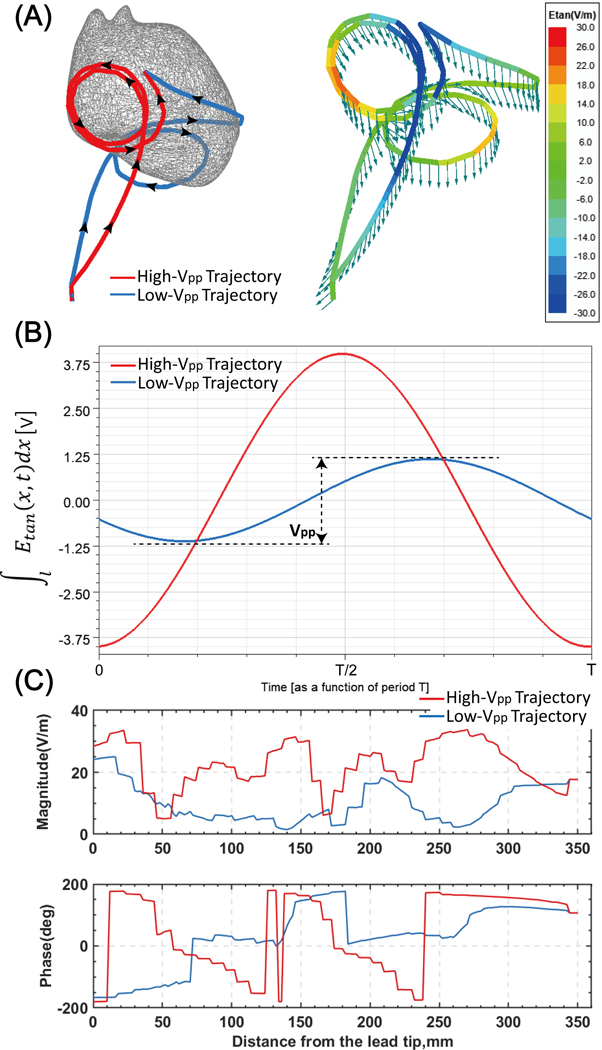
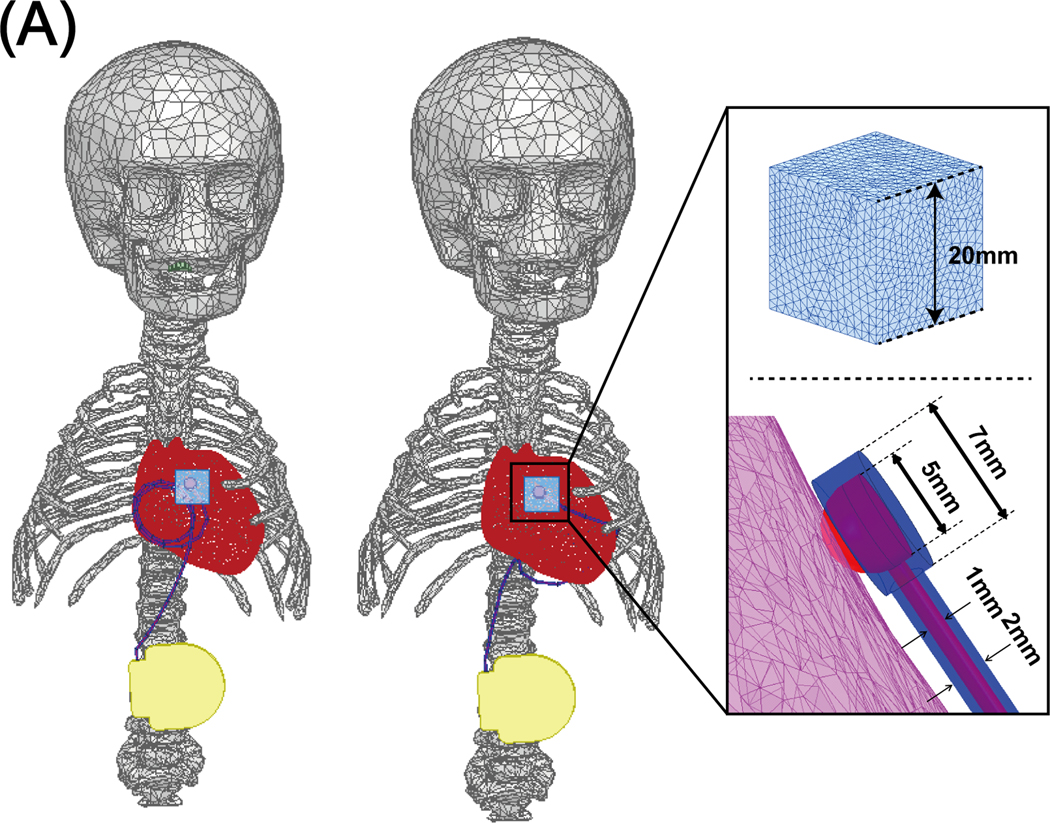
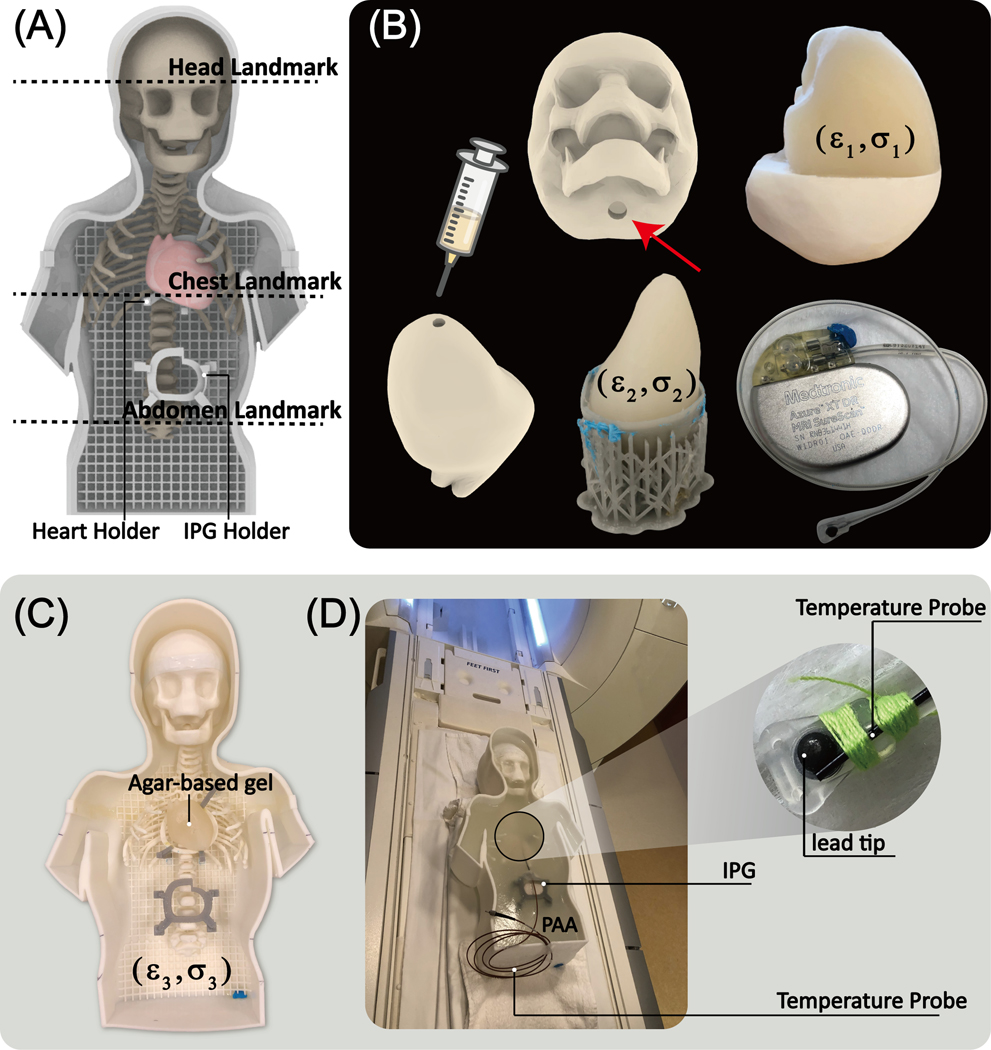
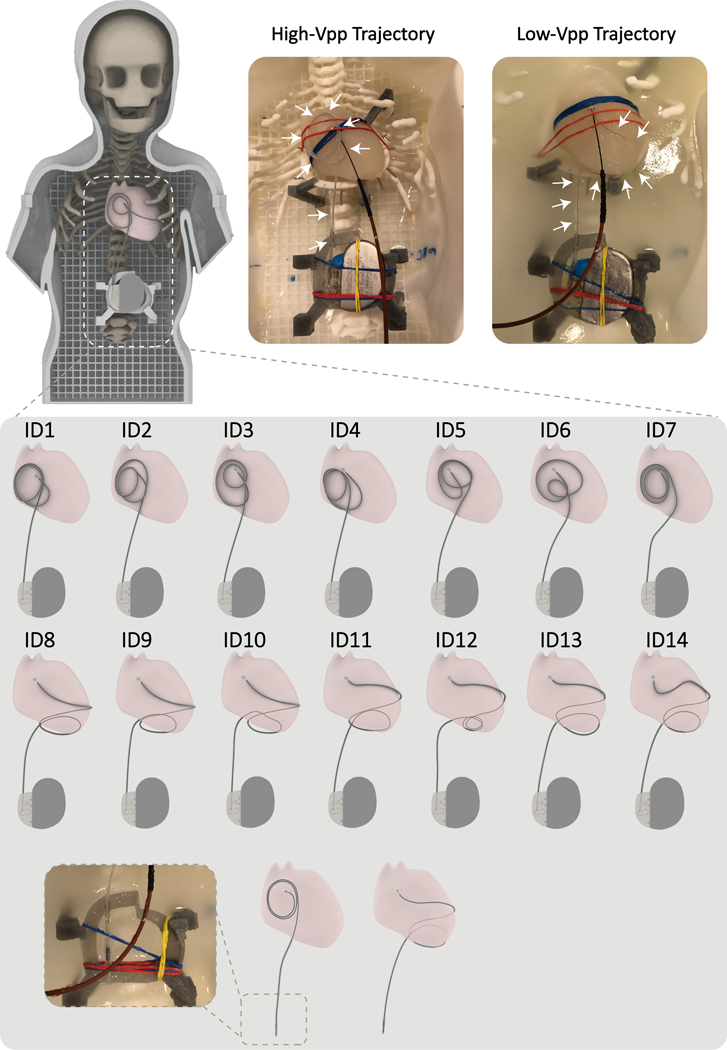
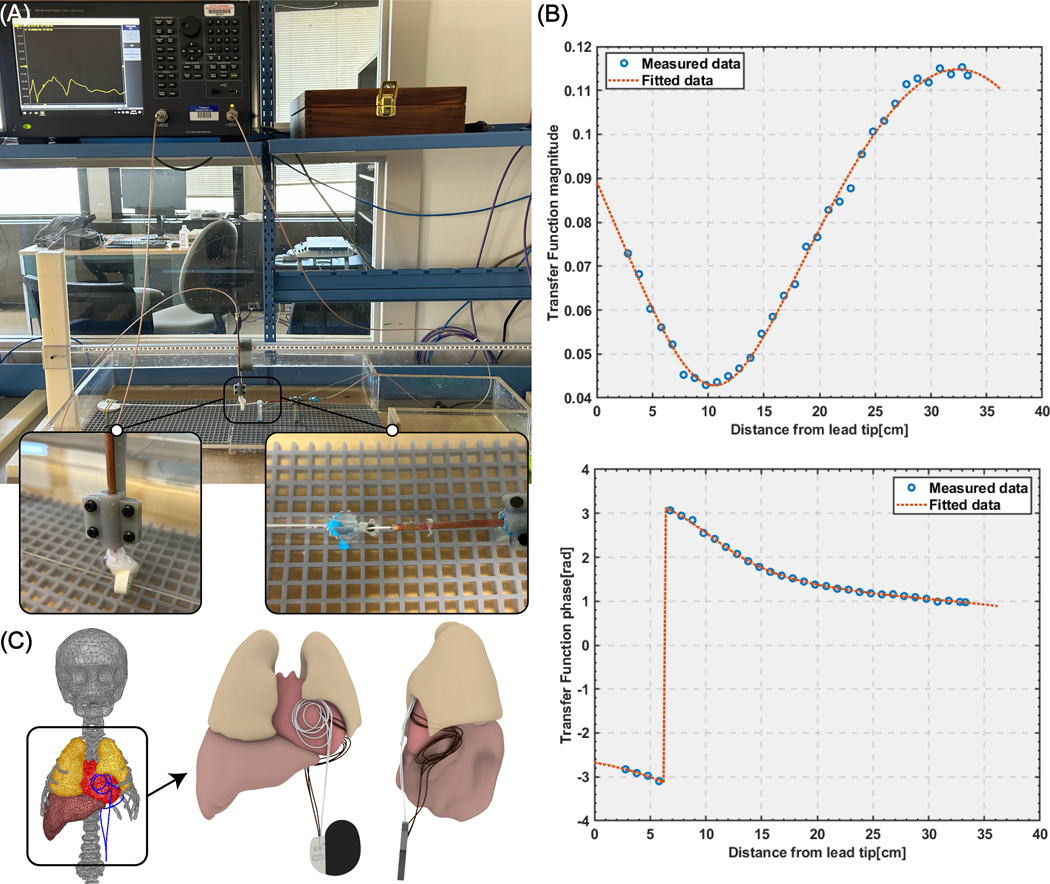
Electromagnetic simulations were performed to assess RF heating of two common 35-cm epicardial lead trajectories exhibiting different degrees of coupling with MRI incident electric fields. Experiments in anthropomorphic phantoms implanted with commercial cardiac implantable electronic devices confirmed the findings. Both electromagnetic simulations and experimental measurements were performed using head-first and feet-first positioning and various landmarks. Transfer function approach was used to assess the performance of suggested modifications in realistic body models.
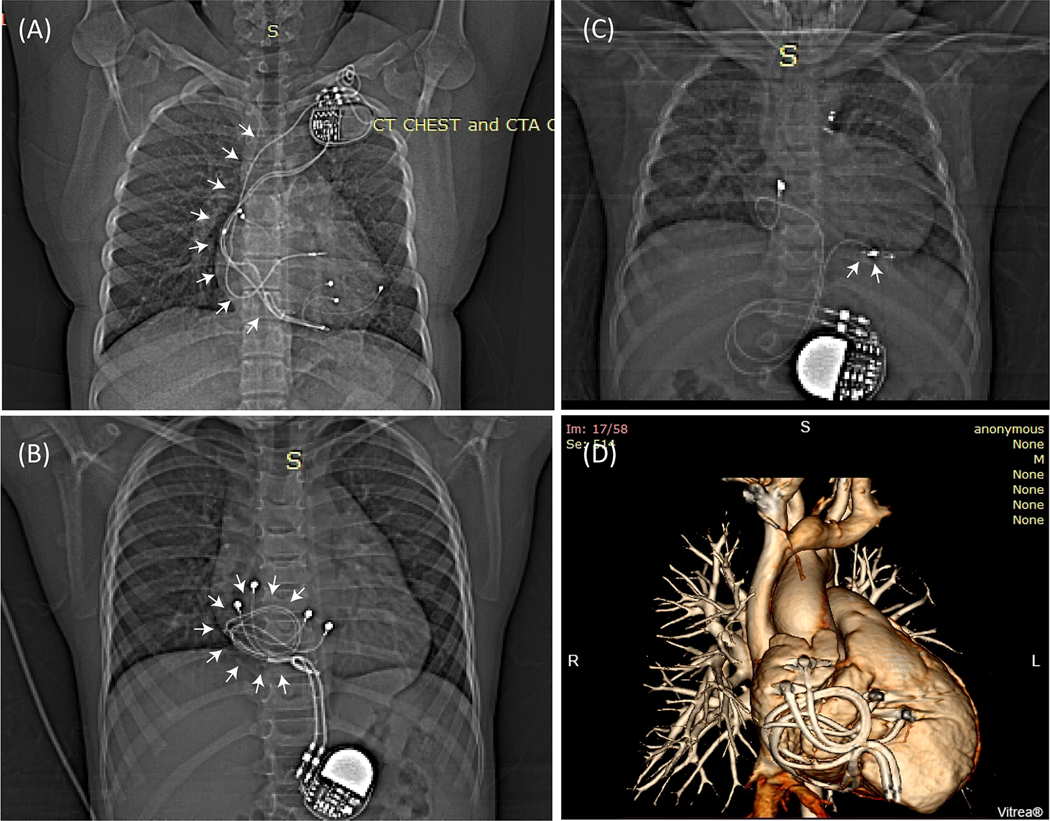
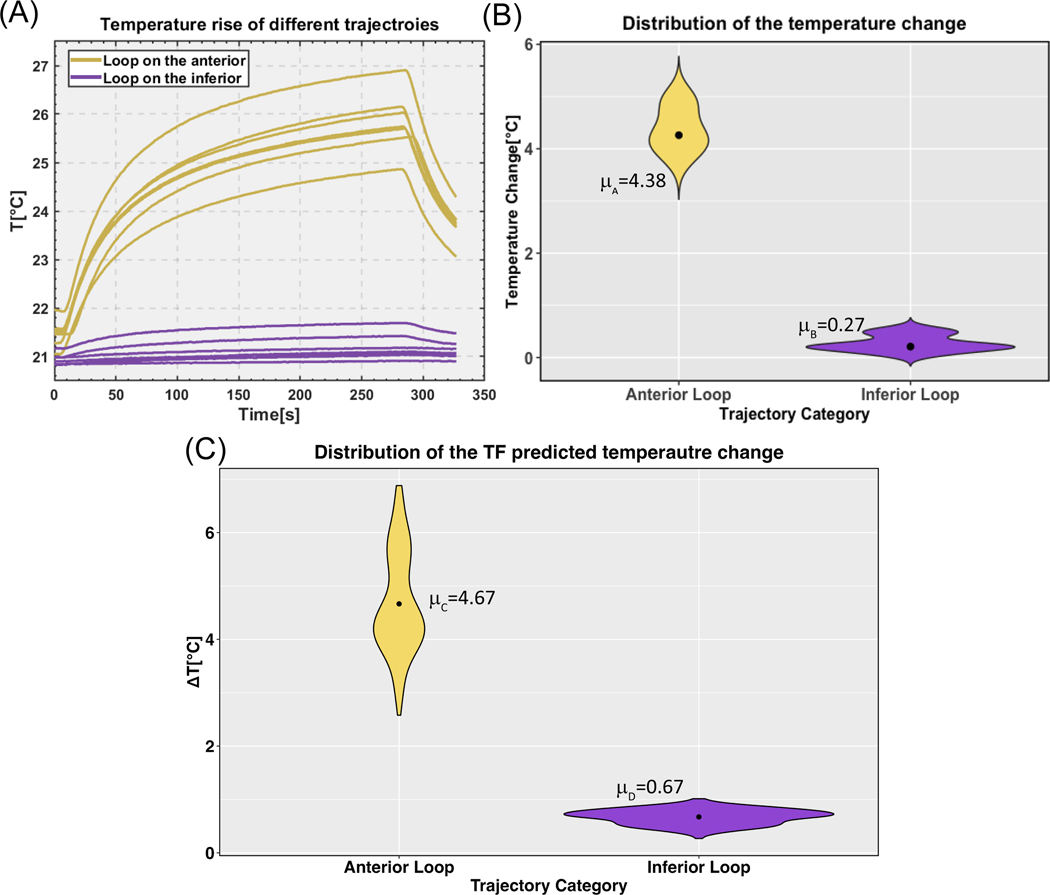
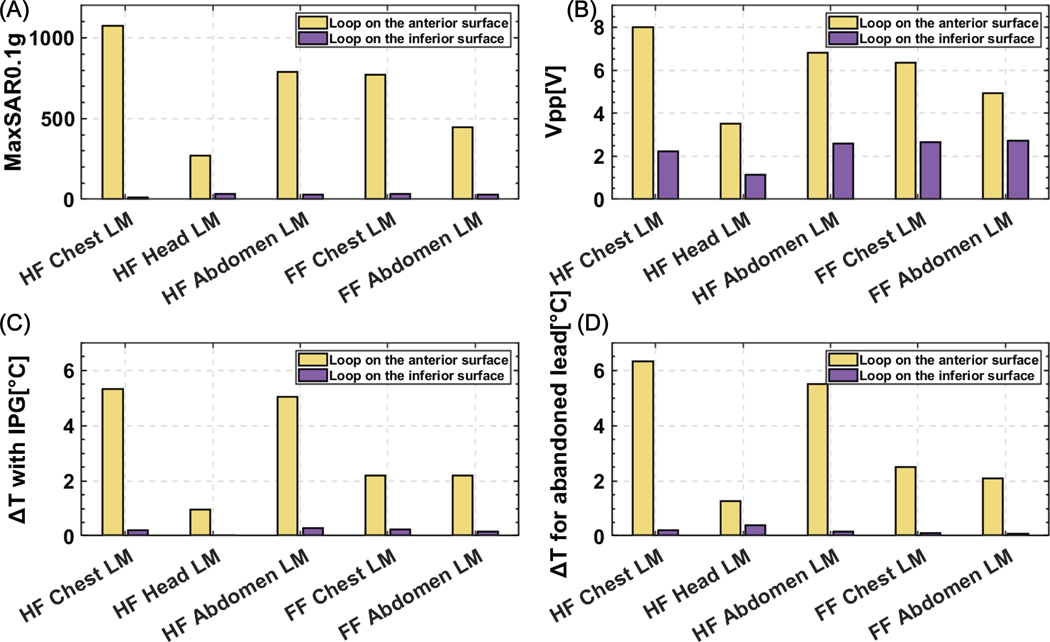
Simulations (head-first, chest landmark) of a 35-cm epicardial lead with a trajectory where the excess length of the lead was looped and placed on the inferior surface of the heart showed an 87-fold reduction in the 0.1 g-averaged specific absorption rate compared with the lead where the excess length was looped on the anterior surface. Repeated experiments with a commercial epicardial device confirmed this. For fully implanted systems following low-specific absorption rate trajectories, there was a 16-fold reduction in the average temperature rise and a 28-fold reduction for abandoned leads. The transfer function method predicted a 7-fold reduction in the RF heating in 336 realistic scenarios.
Surgical modification of epicardial lead trajectory can substantially reduce RF heating at 1.5 T, with benefits extending to abandoned leads.
在儿科患者体内植入心外膜心脏植入式电子设备后,由于射频加热风险增加,他们将无法接受 1.5T MRI 检查。我们研究了在 1.5T 下,通过简单改变心外膜导联的轨迹是否可以显著且可靠地降低 MRI 期间的射频加热,并且这种方法对于废弃导联也同样适用。
进行了电磁场模拟,以评估两种常见的 35cm 心外膜导联轨迹在与 MRI 入射电场不同耦合程度下的射频加热情况。在植入商业心脏植入式电子设备的人体模型中进行了实验,验证了模拟结果。电磁场模拟和实验测量均采用头高脚低位和不同的标志点进行。采用传递函数方法评估了在实际人体模型中对建议修改的性能。
在头高脚低位、胸部标志点进行的 35cm 心外膜导联轨迹模拟中,将多余长度的导联绕成环并放在心脏下表面,与将多余长度的导联绕在心脏前表面的导联相比,0.1g 平均比吸收率降低了 87 倍。商业心外膜设备的重复实验证实了这一点。对于遵循低比吸收率轨迹的完全植入系统,平均温升降低了 16 倍,废弃导联降低了 28 倍。传递函数方法预测,在 336 种实际情况下,射频加热降低了 7 倍。
通过手术改变心外膜导联轨迹可以显著降低 1.5T 下的射频加热,并且这种方法对于废弃导联也同样适用。