Department of Anesthesiology and Pain Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-Ro, Gangnam-Gu, Seoul, 06351, Korea.
Department of Transplantation Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
BMC Anesthesiol. 2023 Aug 5;23(1):263. doi: 10.1186/s12871-023-02208-8.
International guidelines have recommended preemptive kidney transplantation (KT) as the preferred approach, advocating for transplantation before the initiation of dialysis. This approach is advantageous for graft and patient survival by avoiding dialysis-related complications. However, recipients of preemptive KT may undergo anesthesia without the opportunity to optimize volume status or correct metabolic disturbances associated with end-stage renal disease. In these regard, we aimed to investigate the anesthetic events that occur more frequently during preemptive KT compared to nonpreemptive KT.
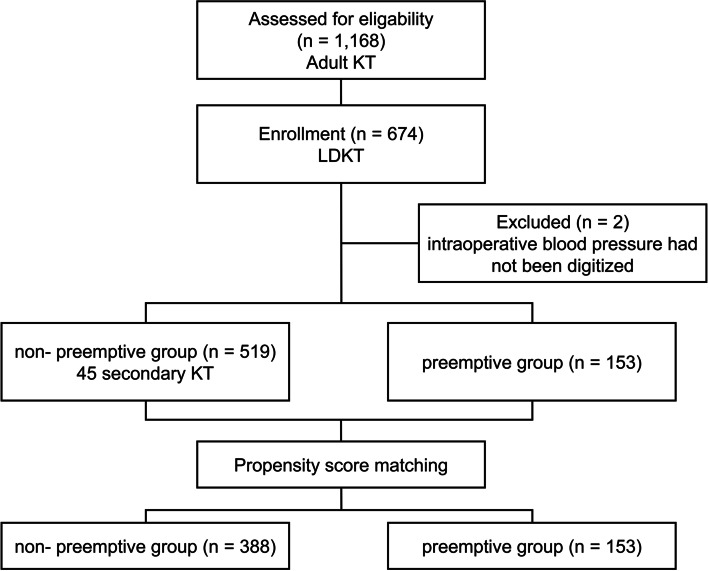
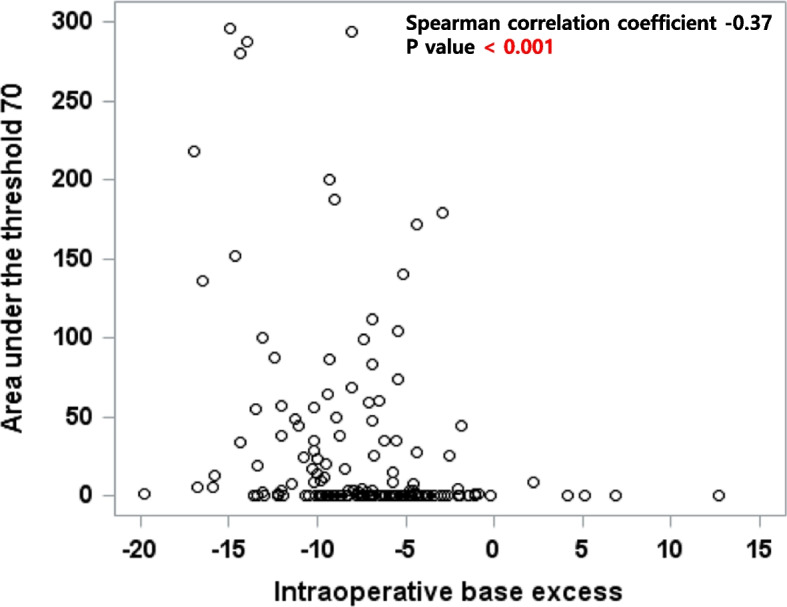
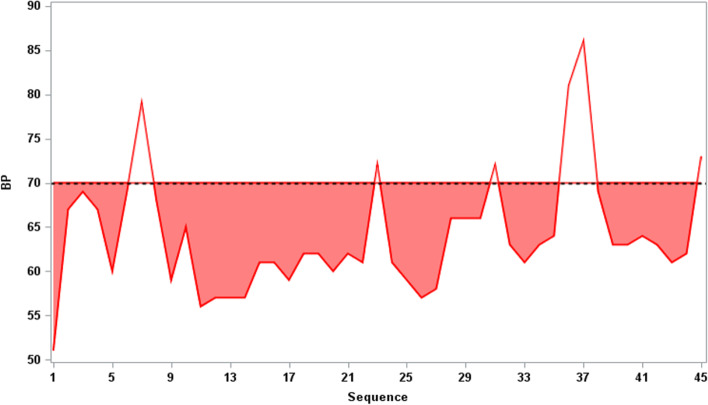
This is a single-center retrospective study. Of the 672 patients who underwent Living donor KT (LDKT), 388 of 519 who underwent nonpreemptive KT were matched with 153 of 153 who underwent preemptive KT using propensity score based on preoperative covariates. The primary outcome was intraoperative hypotension defined as area under the threshold (AUT), with a threshold set at a mean arterial blood pressure below 70 mmHg. The secondary outcomes were intraoperative metabolic acidosis estimated by base excess and serum bicarbonate, electrolyte imbalance, the use of inotropes or vasopressors, intraoperative transfusion, immediate graft function evaluated by the nadir creatinine, and re-operation due to bleeding.
After propensity score matching, we analyzed 388 and 153 patients in non-preemptive and preemptive groups. The multivariable analysis revealed the AUT of the preemptive group to be significantly greater than that of the nonpreemptive group (mean ± standard deviation, 29.7 ± 61.5 and 14.5 ± 37.7, respectively, P = 0.007). Metabolic acidosis was more severe in the preemptive group compared to the nonpreemptive group. The differences in the nadir creatinine value and times to nadir creatinine were statistically significant, but clinically insignificant.
Intraoperative hypotension and metabolic acidosis occurred more frequently in the preemptive group during LDKT. These findings highlight the need for anesthesiologists to be prepared and vigilant in managing these events during surgery.
国际指南建议采用抢先肾移植(KT)作为首选方法,即在开始透析前进行移植。这种方法有利于移植物和患者的存活,避免了与透析相关的并发症。然而,抢先 KT 的受者可能在没有机会优化容量状态或纠正与终末期肾病相关的代谢紊乱的情况下接受麻醉。在这方面,我们旨在研究与非抢先 KT 相比,抢先 KT 中更频繁发生的麻醉事件。
这是一项单中心回顾性研究。在接受活体供肾移植(LDKT)的 672 例患者中,对 519 例未进行抢先 KT 的患者进行了基于术前协变量的倾向评分匹配,共匹配了 153 例进行抢先 KT 的患者。主要结局是术中低血压定义为阈下面积(AUT),阈值设定为平均动脉血压低于 70mmHg。次要结局包括通过碱剩余和血清碳酸氢盐估计的术中代谢性酸中毒、电解质失衡、使用正性肌力药或血管加压药、术中输血、以最低肌酐评估的即刻移植物功能和因出血而再次手术。
在进行倾向评分匹配后,我们对非抢先组和抢先组分别分析了 388 例和 153 例患者。多变量分析显示,抢先组的 AUT 显著大于非抢先组(平均值±标准差,分别为 29.7±61.5 和 14.5±37.7,P=0.007)。抢先组的代谢性酸中毒比非抢先组更严重。最低肌酐值和达到最低肌酐值的时间的差异具有统计学意义,但临床意义不大。
在 LDKT 中,抢先组术中低血压和代谢性酸中毒更频繁发生。这些发现强调了麻醉师在手术中需要准备并警惕这些事件的发生。