McGovern Dominic P, Lees Jennifer S, Traynor Jamie P, Mackinnon Bruce, Bell Samira, Hunter Robert W, Dhaun Neeraj, Metcalfe Wendy, Kidder Dana, Lim Michelle, Joss Nicola, Kelly Michael, Taylor Alison, Cousland Zoe, Dey Vishal, Buck Kate, Brix Silke, Geddes Colin C, McQuarrie Emily P, Stevens Kathryn I
Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow, UK.
Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, UK.
Kidney Int Rep. 2023 Jun 2;8(8):1648-1656. doi: 10.1016/j.ekir.2023.05.029. eCollection 2023 Aug.
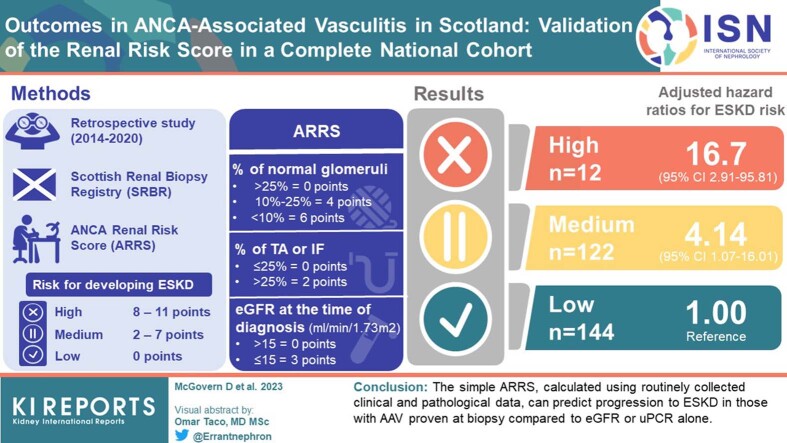
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) causes autoimmune-mediated inflammation of small blood vessels in multiple organs, including the kidneys. The ability to accurately predict kidney outcomes would enable a more personalized therapeutic approach.
We used our national renal biopsy registry to validate the ability of ANCA Renal Risk Score (ARRS) to predict end-stage kidney disease (ESKD) for individual patients. This score uses histopathological and biochemical data to stratify patients as high, medium, or low risk for developing ESKD.
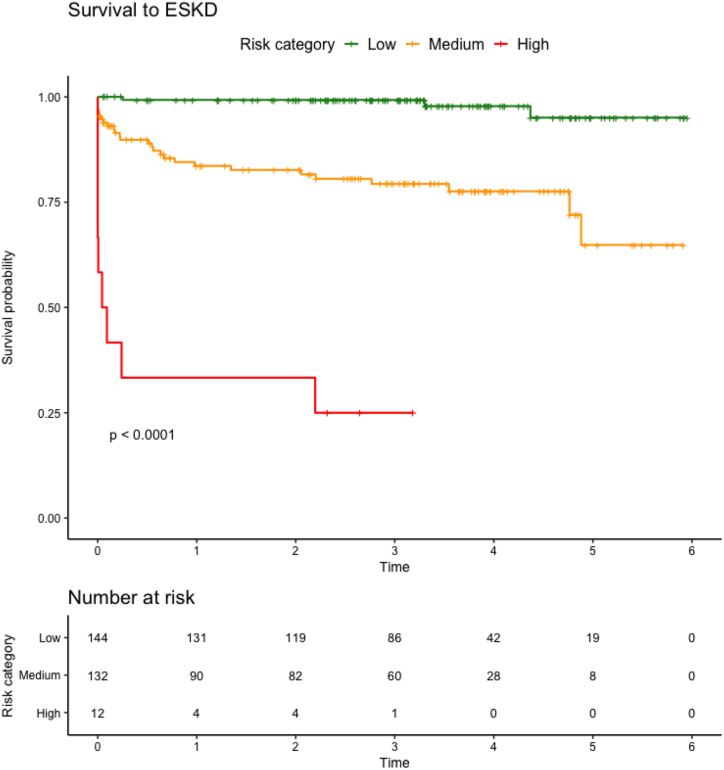
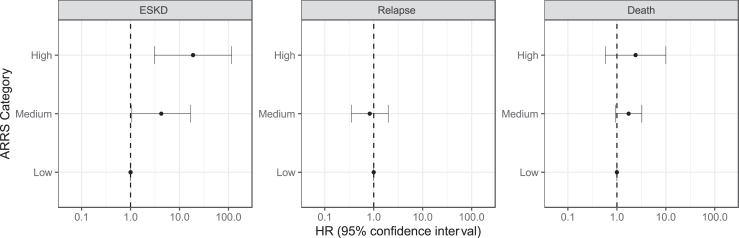
A total of 288 patients were eligible for inclusion in the study (low risk = 144, medium risk = 122, high risk = 12). Using adjusted Cox proportional hazard models with the low-risk group as reference, we show that outcome differs between the categories: high-risk hazard ratio (HR) 16.69 (2.91-95.81, = 0.002); medium risk HR 4.14 (1.07-16.01, = 0.039). Incremental multivariable-adjusted Cox proportional hazards models demonstrated that adding ARRS to a model adjusted for multiple clinical parameters enhanced predictive discrimination (basic model C-statistic 0.864 [95% CI 0.813-0.914], basic model plus ARRS C-statistic 0.877 [95% CI 0.823-0.931]; <0.01).
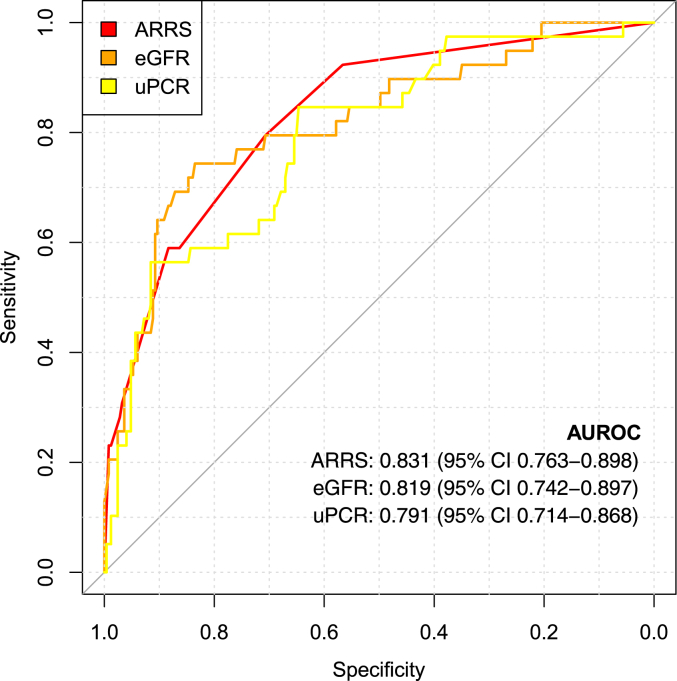
The ARRS better discriminates risk of ESKD in AAV and offers clinicians more prognostic information than the use of standard biochemical and clinical measures alone. This is the first time the ARRS has been validated in a national cohort. The proportion of patients with high-risk scores is lower in our cohort compared to others and should be noted as a limitation of this study.
抗中性粒细胞胞浆抗体(ANCA)相关性血管炎(AAV)可导致包括肾脏在内的多个器官发生自身免疫介导的小血管炎症。准确预测肾脏预后的能力将有助于采取更个性化的治疗方法。
我们利用国家肾脏活检登记处的数据,验证ANCA肾脏风险评分(ARRS)对个体患者终末期肾病(ESKD)的预测能力。该评分使用组织病理学和生化数据将患者分为发生ESKD的高、中、低风险组。
共有288例患者符合纳入本研究的条件(低风险组=144例,中风险组=122例,高风险组=12例)。以低风险组为参照,使用校正后的Cox比例风险模型,我们发现不同类别之间的预后存在差异:高风险组风险比(HR)为16.69(2.91-95.81,P=0.002);中风险组HR为4.14(1.07-16.01,P=0.039)。逐步多变量校正Cox比例风险模型表明,在针对多个临床参数进行校正的模型中加入ARRS可提高预测辨别力(基础模型C统计量为0.864[95%CI 0.813-0.914],基础模型加ARRS的C统计量为0.877[95%CI 0.823-0.931];P<0.01)。
ARRS能更好地辨别AAV患者发生ESKD的风险,与仅使用标准生化和临床指标相比,可为临床医生提供更多预后信息。这是ARRS首次在全国队列中得到验证。与其他研究相比,我们队列中高风险评分患者的比例较低,应将此作为本研究的一个局限性。