Manieri Elisa, Dondi Arianna, Neri Iria, Lanari Marcello
Specialty School of Pediatrics, Alma Mater Studiorum, University of Bologna, Bologna, Italy.
Pediatric Emergency Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Front Med (Lausanne). 2023 Jul 28;10:1108345. doi: 10.3389/fmed.2023.1108345. eCollection 2023.
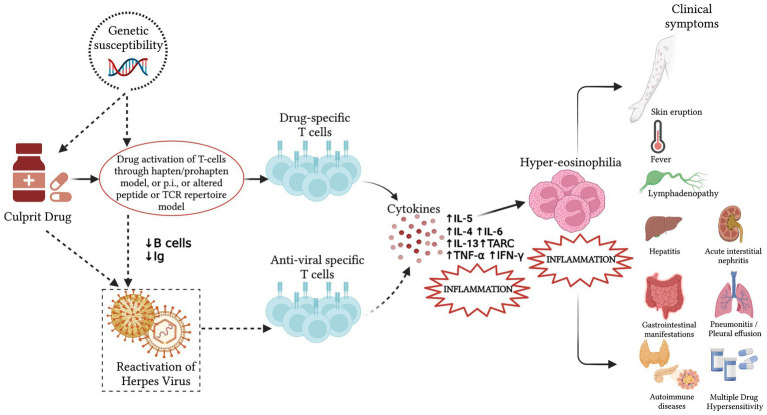
Despite being rare, the Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) syndrome is a serious, possibly fatal condition that may affect both adults and children who may be also burdened by delayed sequelae. It is an adverse drug reaction characterized by widespread skin involvement, fever, lymphadenopathy, visceral involvement, and laboratory abnormalities (eosinophilia, mononucleosis-like atypical lymphocytes). It is more frequently triggered by anticonvulsants, sulphonamides, or antibiotics, the latter being responsible for up to 30% of pediatric cases. The disease typically develops 2-8 weeks after exposure to the culprit medication, with fever and widespread skin eruption; mild viral prodromes are possible. Unfortunately, diagnosis is challenging due to the absence of a reliable test; however, a score by the European Registry of Severe Cutaneous Adverse Reactions (RegiSCAR) allows to classify suspect patients into no, possible, probable, or definite DRESS cases. Moreover, rapid-onset DRESS syndrome has been described in recent years. It affects children more often than adults and differs from the most common form because it appears ≤15 days vs. >15 days after starting the drug, it is usually triggered by antibiotics or iodinated contrast media rather than by anticonvulsants and has a higher presence of lymphadenopathy. Differential diagnosis between rapid-onset antibiotic-driven DRESS syndrome, viral exanthems, or other drug eruptions may be challenging, but it is mandatory to define it as early as possible to start adequate treatment and monitor possible complications. The present review reports the latest evidence about the diagnosis and treatment of pediatric DRESS syndrome.
药物性皮疹伴嗜酸性粒细胞增多和系统症状(DRESS)综合征虽然罕见,但却是一种严重的、可能致命的疾病,可能影响成人和儿童,这些患者还可能受到延迟后遗症的困扰。它是一种药物不良反应,其特征为广泛的皮肤受累、发热、淋巴结病、内脏受累以及实验室检查异常(嗜酸性粒细胞增多、单核细胞增多症样非典型淋巴细胞)。它更常由抗惊厥药、磺胺类药物或抗生素引发,抗生素在儿童病例中占比高达30%。该疾病通常在接触致病药物后2 - 8周出现,伴有发热和广泛的皮疹;可能有轻微的病毒前驱症状。不幸的是,由于缺乏可靠的检测方法,诊断具有挑战性;然而,欧洲严重皮肤不良反应登记处(RegiSCAR)的评分可以将疑似患者分为非DRESS、可能是DRESS、很可能是DRESS或确诊为DRESS病例。此外,近年来还描述了快速起病的DRESS综合征。它在儿童中比成人更常见,与最常见的形式不同,因为它在开始用药后≤15天出现,而不是>15天,通常由抗生素或碘化造影剂引发,而不是抗惊厥药,并且淋巴结病的发生率更高。快速起病的抗生素驱动的DRESS综合征与病毒疹或其他药物疹之间的鉴别诊断可能具有挑战性,但必须尽早明确诊断,以便开始适当的治疗并监测可能的并发症。本综述报告了有关儿童DRESS综合征诊断和治疗的最新证据。