Department of Medicine, Thoracic Oncology Service, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Human Oncology and Pathogenesis Program, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Oncologist. 2023 Nov 2;28(11):978-985. doi: 10.1093/oncolo/oyad197.
Direct KRASG12C inhibitors are approved for patients with non-small cell lung cancers (NSCLC) in the second-line setting. The standard-of-care for initial treatment remains immune checkpoint inhibitors, commonly in combination with platinum-doublet chemotherapy (chemo-immunotherapy). Outcomes to chemo-immunotherapy in this subgroup have not been well described. Our goal was to define the clinical outcomes to chemo-immunotherapy in patients with NSCLC with KRASG12C mutations.
Through next-generation sequencing, we identified patients with advanced NSCLC with KRAS mutations treated with chemo-immunotherapy at 2 institutions. The primary objective was to determine outcomes and determinants of response to first-line chemo-immunotherapy among patients with KRASG12C by evaluating objective response rate (ORR), progression-free survival (PFS), and overall survival (OS). We assessed the impact of coalterations in STK11/KEAP1 on outcomes. As an exploratory objective, we compared the outcomes to chemo-immunotherapy in KRASG12C versus non-G12C groups.
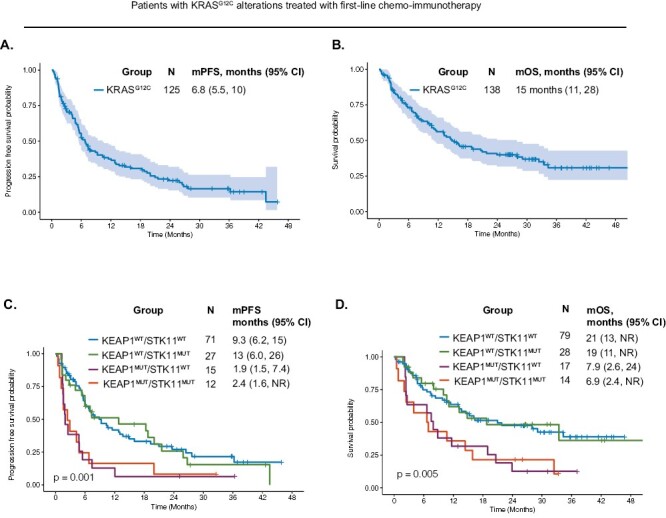
One hundred and thirty eight patients with KRASG12C treated with first-line chemo-immunotherapy were included. ORR was 41% (95% confidence interval (CI), 32-41), median PFS was 6.8 months (95%CI, 5.5-10), and median OS was 15 months (95%CI, 11-28). In a multivariable model for PFS, older age (P = .042), squamous cell histology (P = .008), poor ECOG performance status (PS) (P < .001), and comutations in KEAP1 and STK11 (KEAP1MUT/STK11MUT) (P = .015) were associated with worse PFS. In a multivariable model for OS, poor ECOG PS (P = .004) and KEAP1MUT/STK11MUT (P = .009) were associated with worse OS. Patients with KRASG12C (N = 138) experienced similar outcomes to chemo-immunotherapy compared to patients with non-KRASG12C (N = 185) for both PFS (P = .2) and OS (P = .053).
We define the outcomes to first-line chemo-immunotherapy in patients with KRASG12C, which provides a real-world benchmark for clinical trial design involving patients with KRASG12C mutations. Outcomes are poor in patients with specific molecular coalterations, highlighting the need to develop more effective frontline therapies.
针对非小细胞肺癌(NSCLC)患者,已批准使用直接 KRASG12C 抑制剂进行二线治疗。初始治疗的标准治疗方法仍然是免疫检查点抑制剂,通常与铂类双重化疗(化疗免疫治疗)联合使用。尚未充分描述该亚组接受化疗免疫治疗的结果。我们的目标是确定 KRASG12C 突变的 NSCLC 患者接受化疗免疫治疗的临床结果。
通过下一代测序,我们在 2 个机构确定了接受化疗免疫治疗的晚期 NSCLC 伴 KRAS 突变的患者。主要目的是通过评估客观缓解率(ORR)、无进展生存期(PFS)和总生存期(OS),确定 KRASG12C 患者一线化疗免疫治疗的反应结果和决定因素。我们评估了 STK11/KEAP1 共突变对结果的影响。作为一项探索性目标,我们比较了 KRASG12C 与非 G12C 组接受化疗免疫治疗的结果。
共纳入 138 例接受一线化疗免疫治疗的 KRASG12C 患者。ORR 为 41%(95%CI,32-41),中位 PFS 为 6.8 个月(95%CI,5.5-10),中位 OS 为 15 个月(95%CI,11-28)。在 PFS 的多变量模型中,年龄较大(P=0.042)、鳞状细胞组织学(P=0.008)、较差的 ECOG 表现状态(PS)(P<0.001)和 KEAP1 和 STK11 共突变(KEAP1MUT/STK11MUT)(P=0.015)与较差的 PFS 相关。在 OS 的多变量模型中,较差的 ECOG PS(P=0.004)和 KEAP1MUT/STK11MUT(P=0.009)与较差的 OS 相关。KRASG12C 患者(N=138)与非 KRASG12C 患者(N=185)在 PFS(P=0.2)和 OS(P=0.053)方面均接受了类似的化疗免疫治疗结果。
我们确定了 KRASG12C 患者一线化疗免疫治疗的结果,为涉及 KRASG12C 突变患者的临床试验设计提供了真实世界的基准。具有特定分子共突变的患者预后较差,这突显了开发更有效的一线治疗方法的必要性。