Magnetic Resonance Centre, Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, U.K.
Faculty of Medical Sciences Professional Services, Newcastle University, U.K.
Clin Sci (Lond). 2023 Aug 31;137(16):1333-1346. doi: 10.1042/CS20230586.
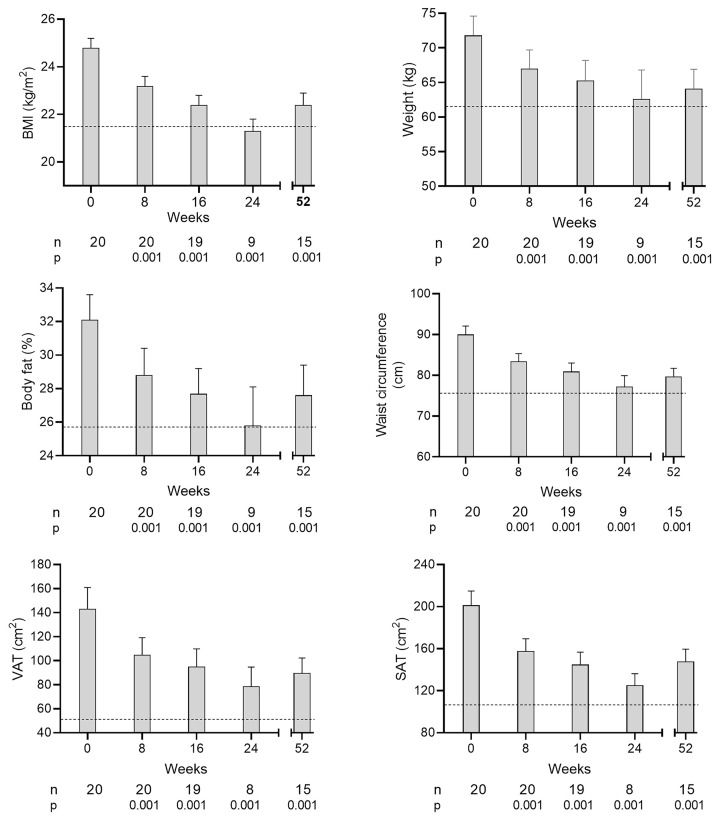
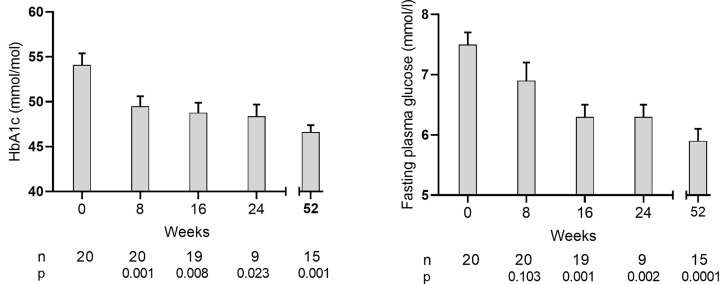
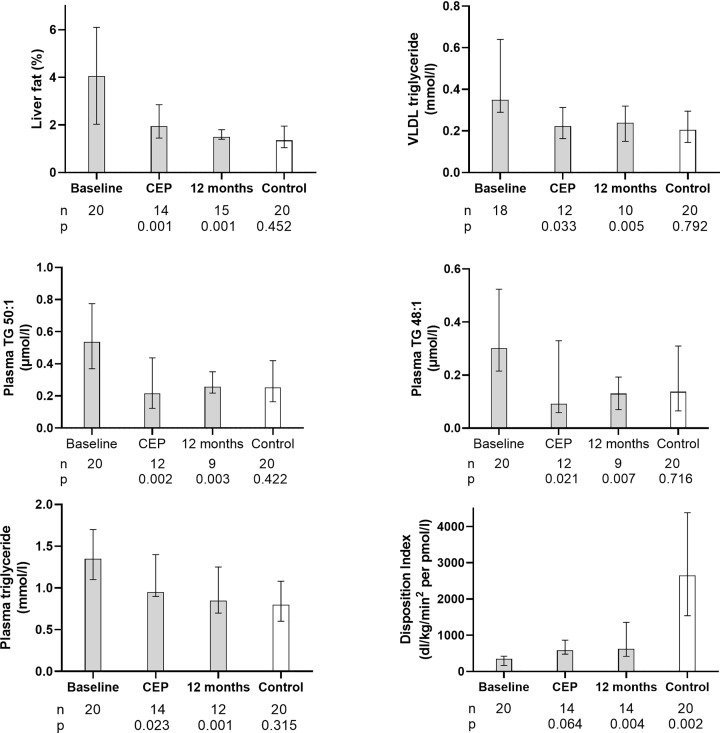
Weight loss in overweight or obese individuals with Type 2 diabetes (T2D) can normalize hepatic fat metabolism, decrease fatty acid oversupply to β cells and restore normoglycaemia. One in six people has BMI <27 kg/m2 at diagnosis, and their T2D is assumed to have different aetiology. The Personal Fat Threshold hypothesis postulated differing individual thresholds for lipid overspill and adverse effects on β-cell function. To test this hypothesis, people with Type 2 diabetes and body mass index <27kg/m2 (n = 20) underwent repeated 5% weight loss cycles. Metabolic assessments were carried out at stable weight after each cycle and after 12 months. To determine how closely metabolic features returned to normal, 20 matched normoglycemic controls were studied once. Between baseline and 12 months: BMI fell (mean ± SD), 24.8 ± 0.4 to 22.5 ± 0.4 kg/m2 (P<0.0001) (controls: 21.5 ± 0.5); total body fat, 32.1 ± 1.5 to 27.6 ± 1.8% (P<0.0001) (24.6 ± 1.5). Liver fat content and fat export fell to normal as did fasting plasma insulin. Post-meal insulin secretion increased but remained subnormal. Sustained diabetes remission (HbA1c < 48 mmol/mol off all glucose-lowering agents) was achieved by 70% (14/20) by initial weight loss of 6.5 (5.5-10.2)%. Correction of concealed excess intra-hepatic fat reduced hepatic fat export, with recovery of β-cell function, glycaemic improvement in all and return to a non-diabetic metabolic state in the majority of this group with BMI <27 kg/m2 as previously demonstrated for overweight or obese groups. The data confirm the Personal Fat Threshold hypothesis: aetiology of Type 2 diabetes does not depend on BMI. This pathophysiological insight has major implications for management.
超重或肥胖 2 型糖尿病(T2D)患者减轻体重可以使肝脂肪代谢正常化,减少脂肪酸对β细胞的过度供应,并恢复正常血糖水平。六分之一的人在诊断时 BMI<27kg/m2,他们的 T2D 被认为具有不同的病因。个人脂肪阈值假说假设不同个体的脂质溢出和对β细胞功能的不良影响有不同的阈值。为了验证这一假说,20 名 BMI<27kg/m2 的 2 型糖尿病患者(n=20)进行了重复的 5%体重减轻周期。在每个周期后和 12 个月时稳定体重下进行代谢评估。为了确定代谢特征恢复正常的程度,还对 20 名匹配的血糖正常对照者进行了一次研究。在基线和 12 个月之间:BMI 下降(均值±标准差),从 24.8±0.4kg/m2 降至 22.5±0.4kg/m2(P<0.0001)(对照组:21.5±0.5);全身脂肪从 32.1±1.5%降至 27.6±1.8%(P<0.0001)(对照组:24.6±1.5)。肝脂肪含量和脂肪输出下降到正常水平,空腹血浆胰岛素也下降到正常水平。餐后胰岛素分泌增加,但仍低于正常水平。通过初始体重减轻 6.5(5.5-10.2)%,70%(14/20)的患者实现了持续的糖尿病缓解(HbA1c<48mmol/mol 且停用所有降糖药物)。纠正隐蔽性肝内脂肪过多减少了肝脂肪输出,恢复了β细胞功能,所有患者的血糖均得到改善,并且大多数 BMI<27kg/m2 的患者恢复到非糖尿病的代谢状态,正如以前超重或肥胖组所证明的那样。这些数据证实了个人脂肪阈值假说:2 型糖尿病的病因并不依赖于 BMI。这种病理生理学的见解对管理具有重大意义。