Research and Development, Yorkshire Ambulance Service NHS Trust, Wakefield, UK
Business Intelligence, NHS Devon, Exeter, UK.
BMJ Open. 2023 Sep 6;13(9):e076203. doi: 10.1136/bmjopen-2023-076203.
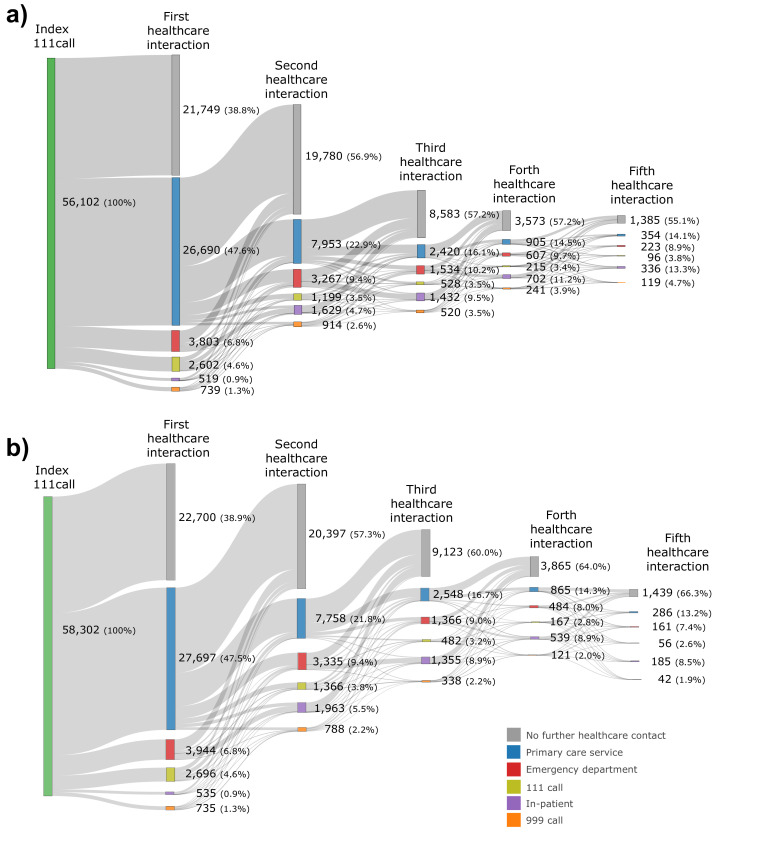
This feasibility study aimed to model in silico the current healthcare system for patients triaged to a primary care disposition following a call to National Health Service (NHS) 111 and determine the effect of reconfiguring the healthcare system to ensure a timely primary care service contact.
Discrete event simulation.
Single English NHS 111 call centre in Yorkshire.
Callers registered with a Bradford general practitioner who contacted the NHS 111 service in 2021 and were triaged to a primary care disposition.
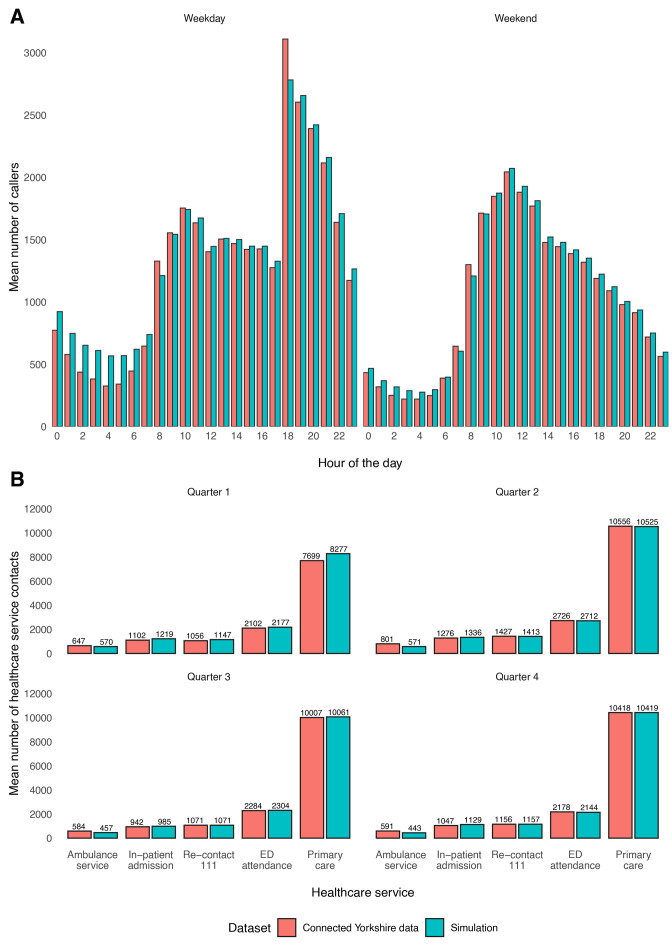
Face validity of conceptual model. Comparison between real and simulated data for quarterly counts (and 95% CIs) for patient contact with emergency ambulance (999), 111, and primary and secondary care services. Mean difference and 95% CIs in healthcare system usage between simulations and difference in mean proportion of avoidable admissions for callers who presented to an emergency department (ED).
The simulation of the current system estimated that there would be 39 283 (95% CI 39 237 to 39 328) primary care contacts, 2042 (95% CI 2032 to 2051) 999 calls and 1120 (95% CI 1114 to 1127) avoidable ED attendances. Modifying the model to ensure a timely primary care response resulted in a mean percentage increase of 196.1% (95% CI 192.2% to 199.9%) in primary care contacts, and a mean percentage decrease of 78.0% (95% CI 69.8% to 86.2%) in 999 calls and 88.1% (95% CI 81.7% to 94.5%) in ED attendances. Avoidable ED attendances reduced by a mean of -26 (95% CI -35 to -17).
In this simulated study, ensuring timely contact with a primary care service would lead to a significant reduction in 999 and 111 calls, and ED attendances (although not avoidable ED attendance). However, this is likely to be impractical given the need to almost double current primary care service provision. Further economic and qualitative research is needed to determine whether this intervention would be cost-effective and acceptable to both patients and primary care clinicians.
本可行性研究旨在对 111 热线转至初级保健的患者当前的医疗保健系统进行计算机模拟,并确定重新配置医疗保健系统以确保及时进行初级保健服务联系的效果。
离散事件模拟。
约克郡的单个英国国民保健服务 111 呼叫中心。
在 2021 年与国民保健服务 111 服务联系并被分诊至初级保健的布拉德福德全科医生注册患者。
概念模型的表面效度。实际数据与模拟数据的季度计数(95%CI)的比较,用于患者与紧急救护车(999)、111 和初级和二级保健服务的接触。模拟与呼叫者到急诊就诊的可避免入院比例差异之间的医疗保健系统使用的平均差异和 95%CI。
当前系统的模拟估计将有 39283(95%CI 39237 至 39328)次初级保健接触、2042(95%CI 2032 至 2051)次 999 呼叫和 1120(95%CI 1114 至 1127)次可避免的 ED 就诊。修改模型以确保及时进行初级保健响应导致初级保健接触的平均百分比增加 196.1%(95%CI 192.2%至 199.9%),999 呼叫的平均百分比减少 78.0%(95%CI 69.8%至 86.2%),ED 就诊的平均百分比减少 88.1%(95%CI 81.7%至 94.5%)。可避免的 ED 就诊减少了平均 26 次(95%CI-35 至-17)。
在这项模拟研究中,确保与初级保健服务及时联系将显著减少 999 和 111 呼叫以及 ED 就诊(尽管不是可避免的 ED 就诊)。然而,鉴于需要将当前的初级保健服务提供增加近一倍,这可能不切实际。需要进一步的经济和定性研究,以确定这种干预措施是否具有成本效益,并且对患者和初级保健临床医生都是可以接受的。