Department of Biomedical and Clinical Sciences, Linköping University, Linköping, 581 85, Sweden.
Department of Translational Medicine - Hand Surgery, Lund University, Malmö, 205 02, Sweden.
BMC Musculoskelet Disord. 2023 Sep 7;24(1):713. doi: 10.1186/s12891-023-06838-4.
Benign peripheral nerve tumours consist of different types, most commonly Schwannomas. Preoperative Magnetic Resonance Imaging (MRI) is commonly performed before surgery and Pathoanatomical Diagnosis (PAD) confirms the diagnosis. Our aims were to study the utility of MRI and the relation between tumour size and symptoms.
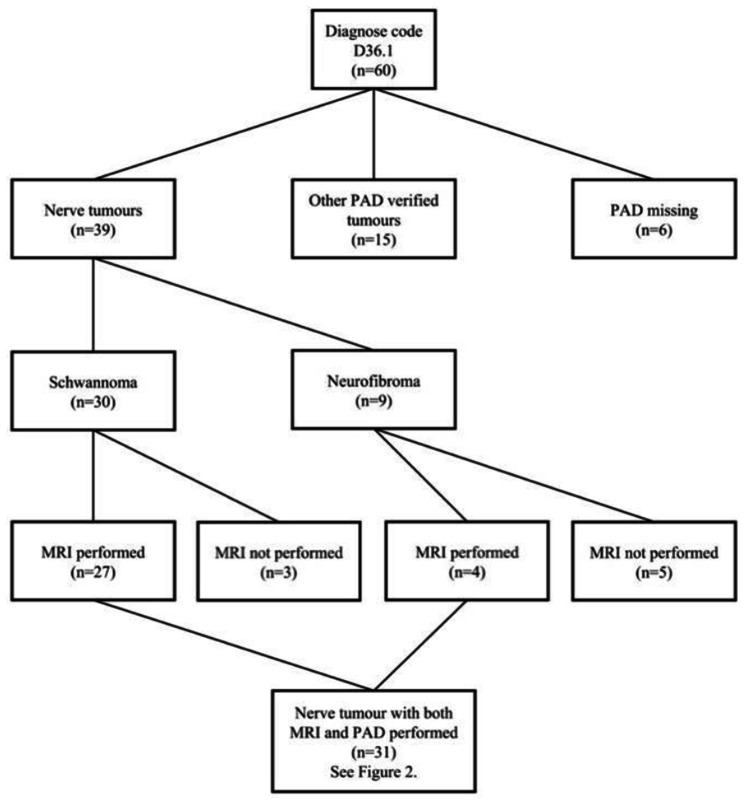
Retrospectively, patients, surgically treated for benign nerve tumours between 2008 and 2019, were identified and preoperative MRI, with measurement of tumour size, PAD, symptoms, peroperative details, and symptomatic outcomes of surgery, were analysed.
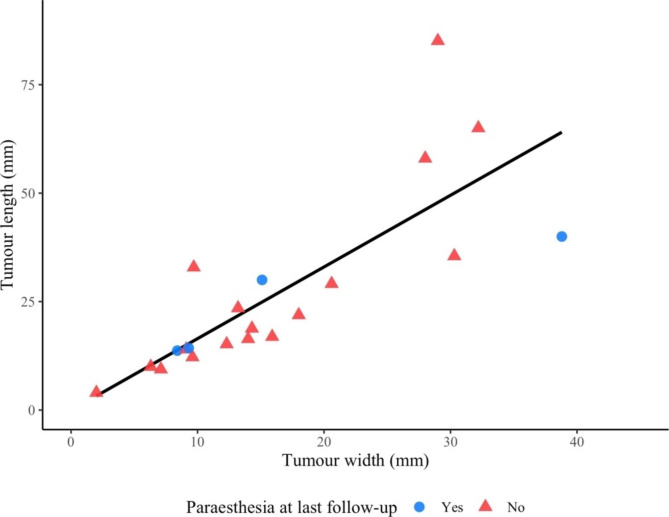
The sensitivity and specificity to correctly identify Schwannomas with preoperative MRI were 85% and 50%, respectively, based on 30 Schwannomas and nine neurofibromas that were identified. Tumour size did not affect the presence of preoperative symptoms, but patients with sensory dysfunction at last follow-up had larger Schwannomas (p < 0.05). Symptoms as a palpable tumour, paraesthesia and pain improved by surgical excision (p < 0.001, p < 0.001 and p < 0.012, respectively), but sensory and motor dysfunction were common postoperatively. No malignant peripheral nerve sheath tumours (MPNST) were found. Using a surgical microscope, instead of only loop magnification, lowered the risk of perioperative nerve injuries (p < 0.05), but did not further diminish postoperative symptoms.
Early and accurate diagnosis of Schwannomas is valuable for adequate presurgical preparation and prompt surgical intervention. Preoperative examination with MRI has a high sensitivity, but low specificity; although recent advancement in MRI technology indicates improvement in diagnostic precision. Surgical excision is preferably performed early in conjunction with symptomatic debut to improve outcome.
良性周围神经肿瘤包括多种类型,最常见的是神经鞘瘤。术前磁共振成像(MRI)常用于手术前,病理解剖诊断(PAD)可确诊。我们的目的是研究 MRI 的效用以及肿瘤大小与症状之间的关系。
回顾性分析 2008 年至 2019 年间接受良性神经肿瘤手术治疗的患者,分析术前 MRI(测量肿瘤大小)、PAD、症状、手术过程中的详细情况以及手术的症状转归。
术前 MRI 正确识别神经鞘瘤的敏感性和特异性分别为 85%和 50%,共识别出 30 个神经鞘瘤和 9 个神经纤维瘤。肿瘤大小与术前症状的出现无关,但最后随访时感觉功能障碍患者的神经鞘瘤较大(p<0.05)。作为可触及的肿瘤、感觉异常和疼痛的症状通过手术切除得到改善(p<0.001、p<0.001 和 p<0.012),但术后常出现感觉和运动功能障碍。未发现恶性周围神经鞘瘤(MPNST)。与仅使用环式放大相比,使用手术显微镜降低了围手术期神经损伤的风险(p<0.05),但并不能进一步减轻术后症状。
早期、准确地诊断神经鞘瘤对于充分的术前准备和及时的手术干预是有价值的。术前 MRI 检查具有较高的敏感性,但特异性较低;尽管 MRI 技术的最新进展表明其诊断精度有所提高。手术切除最好与症状出现早期进行,以改善预后。