Desmond Tutu HIV Centre, Institute of Infectious Diseases and Molecular Medicine and Department of Medicine, University of Cape Town, Cape Town, South Africa.
University of Colorado, Aurora, CO, USA.
AIDS Res Ther. 2023 Sep 14;20(1):67. doi: 10.1186/s12981-023-00552-w.
Suboptimal antiretroviral (ART) adherence can lead to virologic failure with consequent HIV-1 resistance. Tenofovir diphosphate (TFV-DP) in dried blood spots (DBS) is a powerful biomarker of cumulative adherence, predictive of future viremia. It has been associated with resistance in Persons With HIV (PWH) in South Africa and the US. We explored the relationship of TFV-DP concentrations with antiretroviral drug resistance at the time of treatment failure in SA.
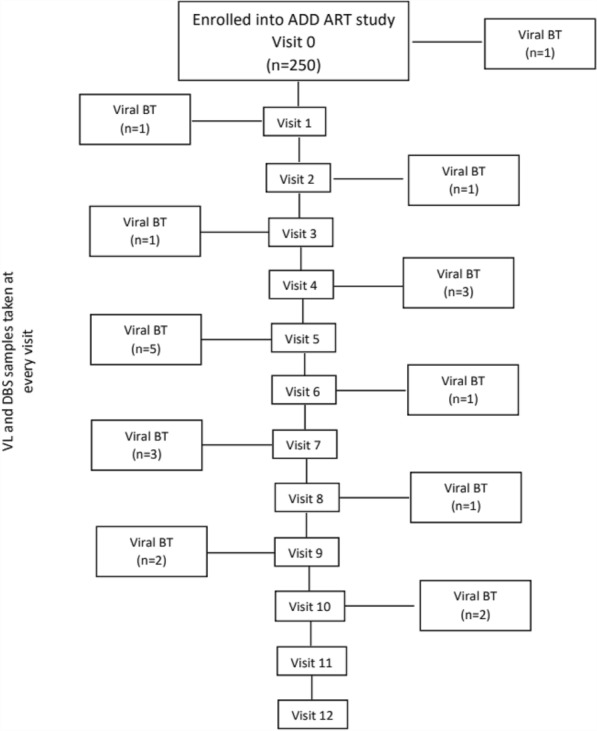
Adult PWH from health clinics in Cape Town, South Africa on efavirenz-based first-line ART containing tenofovir disoproxil fumarate (TDF) with an undetectable (< 50 copies/mL) HIV-1 viral load (VL) were prospectively enrolled in an observational cohort for 12 months. Monthly study visits included blood collection for HIV-1 VL and DBS for TFV-DP. The first confirmed viral breakthrough (VB) > 400 copies/mL triggered HIV-1 genotyping at the subsequent visit. An electronic adherence (EA) device monitored ART adherence in real-time, estimated as a percent for the 30-days prior to VB. Wilcoxon rank sum test was used to compare median [IQR] TFV-DP by genotype outcome.
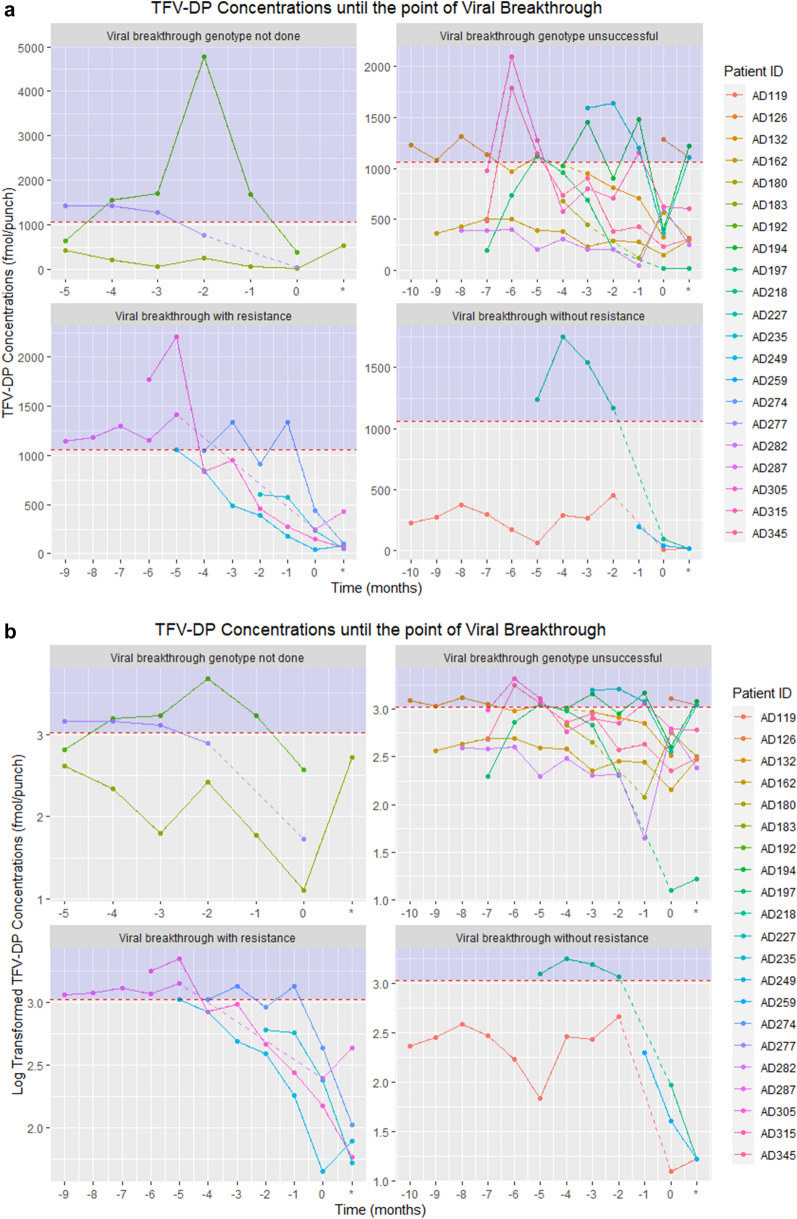
Of 250 individuals, (n = 195, 78% women), 21 experienced VB, with a median of 5 [4;7] months on study, and a median EA of 33.3 [13.3;53.3]%. Demographic characteristics between those with and without VB were similar. Median VL at VB was 4.0 [3.2;4.5] log copies/mL. TFV-DP concentrations trended down towards the VB visit. Median TFV-DP concentrations were significantly higher in those HIV-1 genotype did not amplify due to being virally suppressed at the subsequent visit (n = 10; 380 [227-661] fmol/punch, p = 0.035; EA 45 [24.9; 59.2]%); than in those who were successfully genotyped with evidence of drug resistance (n = 5, 241 [150-247] fmol/punch, EA 20 [6.7;36.7]%) and in individuals who did not have resistance (n = 3, 39.9 [16.6; 93.9] fmol/punch; EA 33.3 [16-38]%). Three genotype collections were not done. Only non-nucleoside reverse transcriptase inhibitor-associated mutations were identified on resistance testing. (K103N, E138K, Y118H).
TFV-DP in DBS showed a step-wise inverse relationship with VB and drug resistance, with evidence of low cumulative ART adherence in PWH who developed antiretroviral resistance. Monitoring TFV-DP concentrations could be a valuable tool for predicting future VB and future resistance.
抗逆转录病毒(ART)治疗依从性不佳可导致病毒学失败,进而导致 HIV-1 耐药。干血斑(DBS)中的替诺福韦二磷酸(TFV-DP)是累积治疗依从性的有力生物标志物,可预测未来的病毒血症。它与南非和美国的 HIV 感染者(PWH)的耐药性有关。我们探讨了在南非治疗失败时,TFV-DP 浓度与抗逆转录病毒药物耐药性之间的关系。
来自南非开普敦诊所的接受基于依非韦伦的一线 ART 的成年 PWH,该 ART 含有替诺福韦二吡呋酯(TDF),HIV-1 病毒载量(VL)不可检测(<50 拷贝/mL),前瞻性纳入了一个为期 12 个月的观察队列。每月的研究访问包括采集 HIV-1 VL 和 DBS 以检测 TFV-DP。首次确认的病毒突破(VB)>400 拷贝/mL 会在随后的就诊时触发 HIV-1 基因分型。电子依从性(EA)设备实时监测 ART 依从性,估计 VB 前 30 天的百分比。Wilcoxon 秩和检验用于比较基因型结果的中位数[IQR]TFV-DP。
在 250 名参与者中(n=195,78%为女性),21 名发生 VB,中位研究时间为 5[4;7]个月,中位 EA 为 33.3[13.3;53.3]%。发生 VB 与未发生 VB 的参与者的人口统计学特征相似。VB 时的中位 VL 为 4.0[3.2;4.5]log 拷贝/mL。TFV-DP 浓度在 VB 就诊时呈下降趋势。随后就诊时病毒抑制的 HIV-1 基因型未扩增的参与者(n=10)的 TFV-DP 浓度中位数明显较高(380[227-661]fmol/刺,p=0.035;EA 45[24.9;59.2]%),而成功进行基因分型且有耐药证据的参与者(n=5,241[150-247]fmol/刺,EA 20[6.7;36.7]%)和无耐药的参与者(n=3,39.9[16.6;93.9]fmol/刺;EA 33.3[16-38]%)。有 3 个基因型未采集。耐药检测仅发现非核苷类逆转录酶抑制剂相关突变(K103N、E138K、Y118H)。
DBS 中的 TFV-DP 与 VB 和耐药性呈逐步反向关系,提示在发生抗病毒耐药的 HIV 感染者中存在累积 ART 依从性低的证据。监测 TFV-DP 浓度可能是预测未来 VB 和未来耐药性的有价值工具。