Cao Kexin, Wu Xiaoyue, Yang Mengya, Chen Can, Zhang Xiaobao, Jiang Daixi, Du Yuxia, Chen Mengsha, You Yue, Zhou Wenkai, Qi Jiaxing, Chen Dingmo, Yan Rui, Miao Ziping, Yang Shigui
Department of Emergency Medicine, Second Affiliated Hospital, Department of Public Health, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, The Key Laboratory of Intelligent Preventive Medicine of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China.
Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, China.
Front Public Health. 2023 Sep 7;11:1243408. doi: 10.3389/fpubh.2023.1243408. eCollection 2023.
Several studies have reported on hepatitis E virus (HEV) prevalence in various regions of China, but the results vary widely. Herein, we conducted a systematic review and meta-analysis to assess the seroprevalence, RNA-positive rate, genotype distribution of HEV in China, and its risk factors.
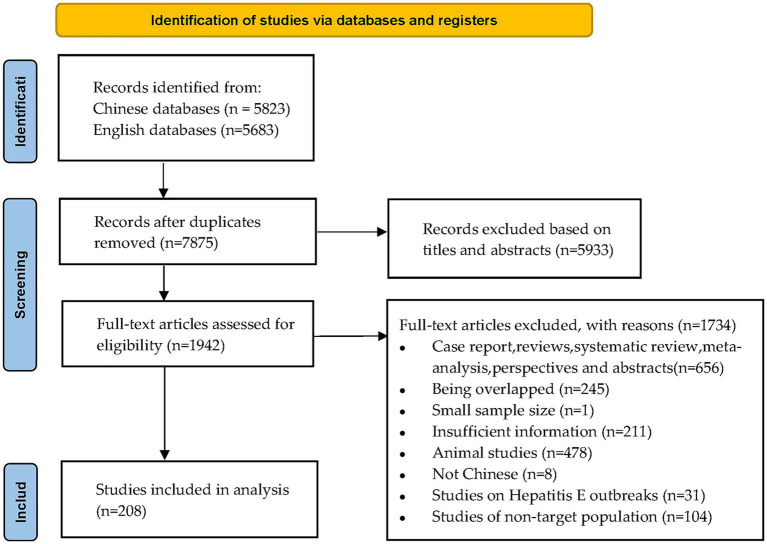
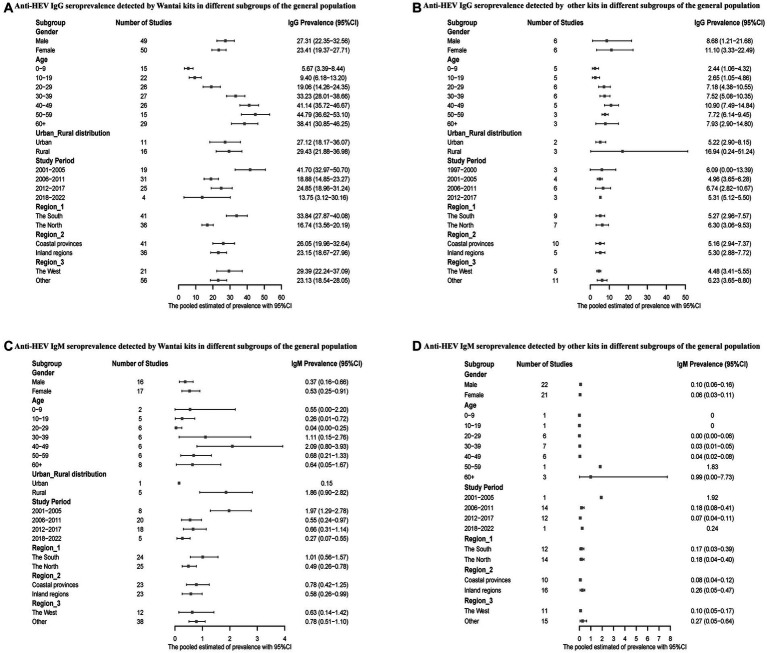
We included 208 related studies involving 1,785,569 participants published between 1997 and 2022. Random-effects models were used to pool prevalence, and subgroup analyses were conducted by population, gender, age, study period, regions, and rural-urban distribution. The meta regression models and pooled odds ratios (OR) were performed to identify risk factors for HEV infections.
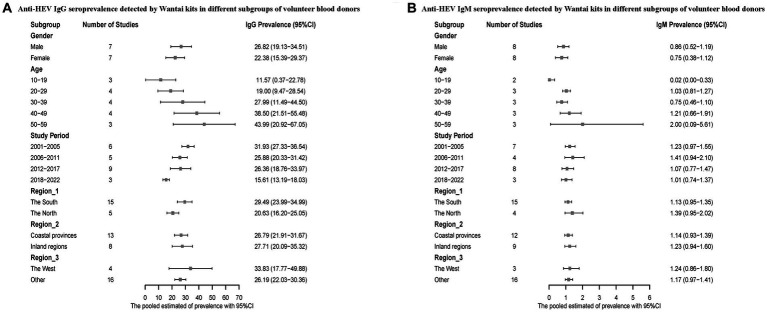
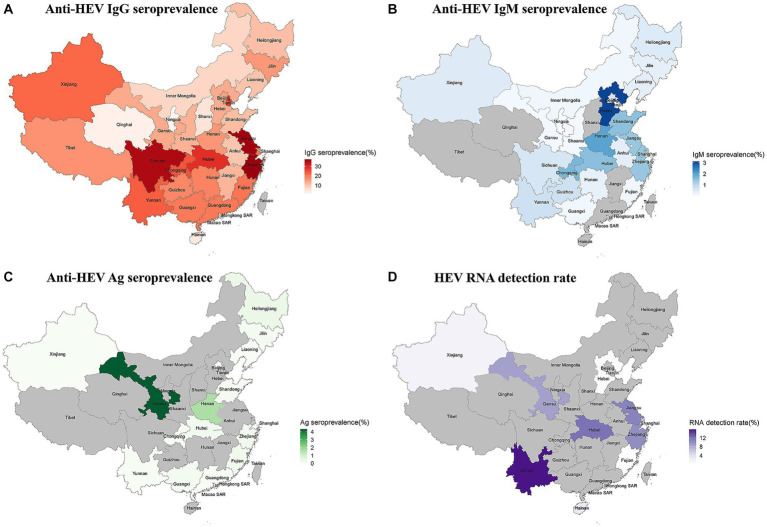
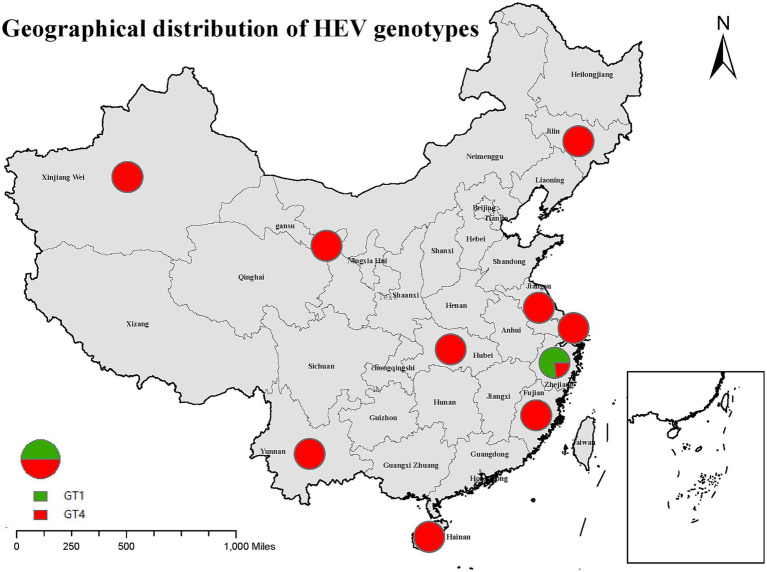
The pooled anti-HEV IgG, IgM, and Ag seroprevalence, and RNA detection rates in China from 1997 to 2022 were 23.17% [95% confidence interval (CI): 20.23-26.25], 0.73% (95% CI: 0.55-0.93), 0.12% (95% CI: 0.01-0.32), and 6.55% (95% CI: 3.46-12.05), respectively. The anti-HEV IgG seropositivity was higher in the occupational population (48.41%; 95% CI: 40.02-56.85) and older adult aged 50-59 years (40.87%; 95% CI: 31.95-50.11). The dominant genotype (GT) of hepatitis E in China was GT4. Notably, drinking non-tap water (OR = 1.82; 95% CI: 1.50-2.20), consumption of raw or undercooked meat (OR = 1.47; 95% CI: 1.17-1.84), and ethnic minorities (OR = 1.50; 95% CI: 1.29-1.73) were risk factors of anti-HEV IgG seroprevalence.
Overall, the prevalence of hepatitis E was relatively high in China, especially among older adults, ethnic minorities, and humans with occupational exposure to pigs. Thus, there is a need for preventive measures, including HEV infection screening and surveillance, health education, and hepatitis E vaccine intervention in high-risk areas and populations.
https://www.crd.york.ac.uk/prospero/, identifier CRD42023397036.
多项研究报告了中国不同地区戊型肝炎病毒(HEV)的流行情况,但结果差异很大。在此,我们进行了一项系统评价和荟萃分析,以评估中国HEV的血清流行率、RNA阳性率、基因型分布及其危险因素。
我们纳入了1997年至2022年发表的208项相关研究,涉及1,785,569名参与者。采用随机效应模型汇总流行率,并按人群、性别、年龄、研究时期、地区和城乡分布进行亚组分析。进行元回归模型和合并比值比(OR)分析以确定HEV感染的危险因素。
1997年至2022年中国抗HEV IgG、IgM和Ag的合并血清流行率以及RNA检测率分别为23.17%[95%置信区间(CI):20.23 - 26.25]、0.73%(95%CI:0.55 - 0.93)、0.12%(95%CI:0.01 - 0.32)和6.55%(95%CI:3.46 - 12.05)。职业人群(48.41%;95%CI:40.02 - 56.85)和50 - 59岁的老年人(40.87%;95%CI:31.95 - 50.11)的抗HEV IgG血清阳性率较高。中国戊型肝炎的主要基因型(GT)为GT4。值得注意的是,饮用非自来水(OR = 1.82;95%CI:1.50 - 2.20)、食用生肉或未煮熟的肉(OR = 1.47;95%CI:1.17 - 1.84)以及少数民族(OR = 1.50;95%CI:1.29 - 1.73)是抗HEV IgG血清流行率的危险因素。
总体而言,中国戊型肝炎的流行率相对较高,尤其是在老年人、少数民族以及职业接触猪的人群中。因此,需要采取预防措施,包括在高危地区和人群中进行HEV感染筛查和监测、健康教育以及戊型肝炎疫苗干预。