Institut Clínic Cardiovascular, Hospital Clínic, Universitat de Barcelona, Carrer Villaroel, 170, 08036 Barcelona, Catalonia, Spain.
Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Universitat de Barcelona, Carrer del Rosselló, 149, 08036 Barcelona, Catalonia, Spain.
Europace. 2023 Aug 2;25(9). doi: 10.1093/europace/euad276.
Recurrence of arrhythmia after catheter ablation of atrial fibrillation (AF) in the form of atypical atrial flutter (AFL) is common among a significant number of patients and often requires redo ablation with limited success rates. Identifying patients at high risk of AFL after AF ablation could aid in patient selection and personalized ablation approach. The study aims to assess the relationship between pre-existing atrial cardiomyopathy and the occurrence of AFL following AF ablation.
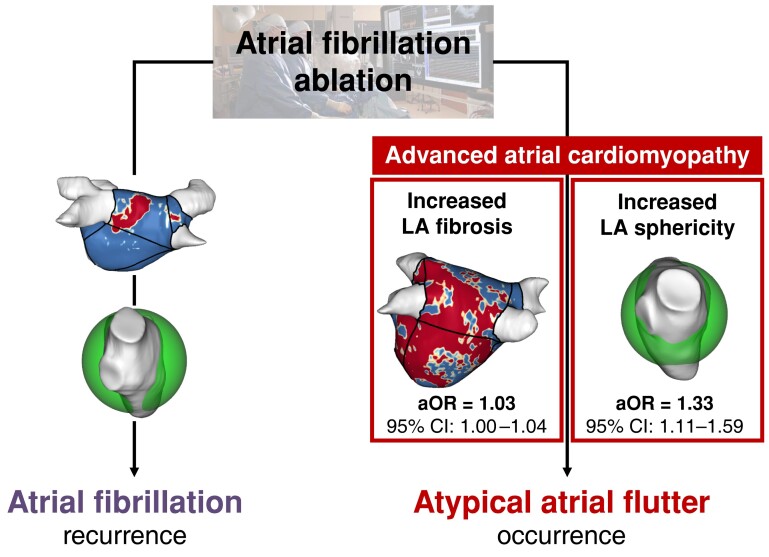
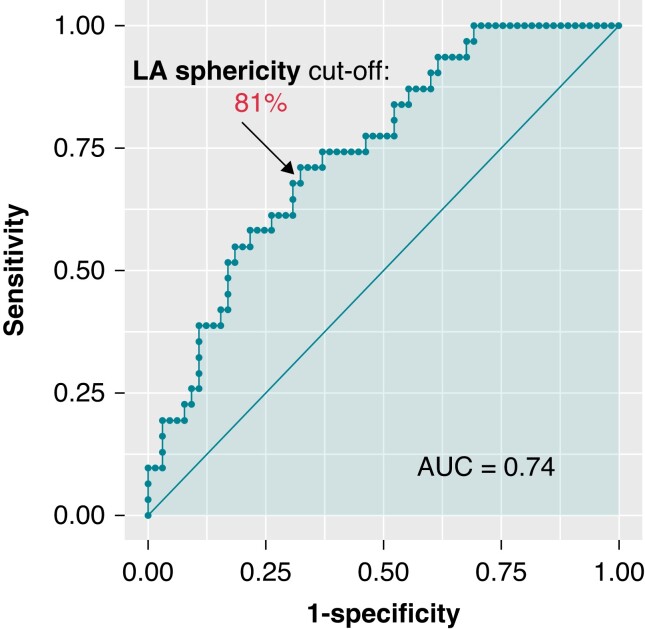
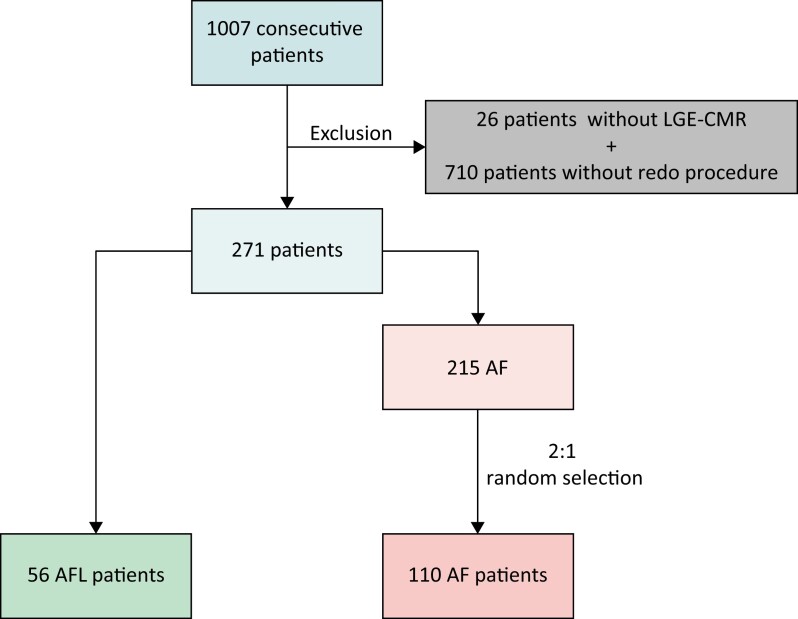
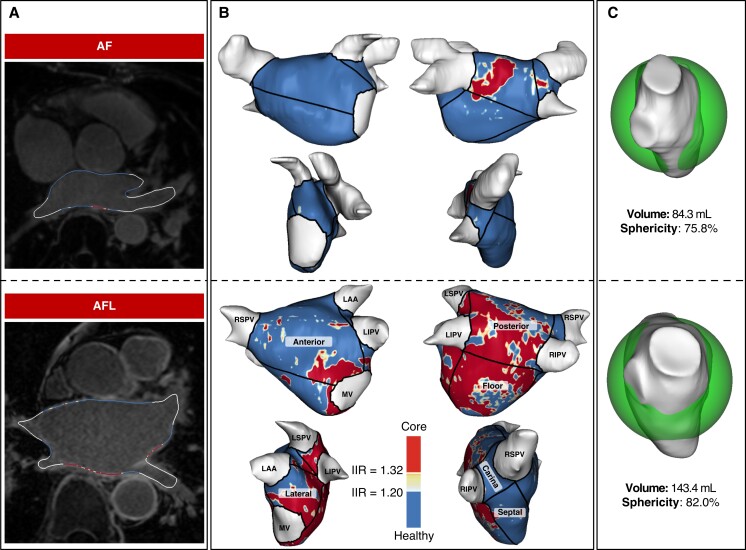
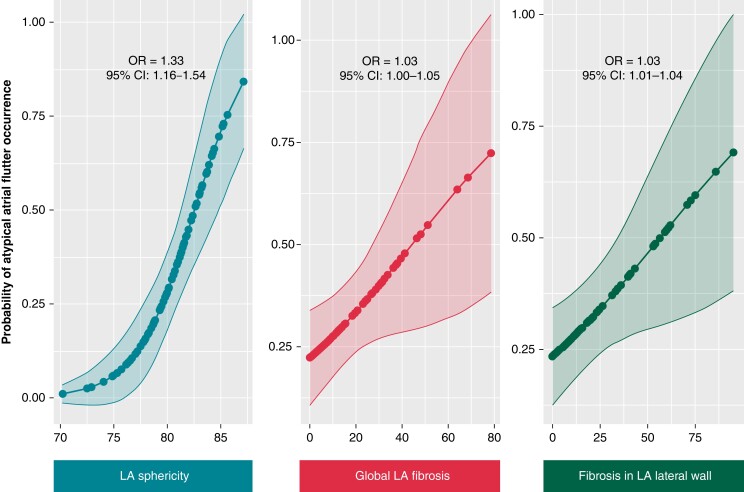
We analysed a cohort of 1007 consecutive AF patients who underwent catheter ablation and were included in a prospective registry. Patients who did not have baseline cardiac magnetic resonance imaging and late gadolinium enhancement (LGE-CMR) or did not experience any recurrences were excluded. A total of 166 patients were included gathering 56 patients who underwent re-ablation due to AFL recurrences and 110 patients who underwent re-ablation due to AF recurrences (P = 0.11). A multiparametric assessment of atrial cardiomyopathy was based on basal LGE-CMR, including left atrial (LA) volume, LA sphericity, and global and segmental LA fibrosis using semiautomated post-processing software. Out of the initial cohort of 1007 patients, AFL and AF occurred in 56 and 110 patients, respectively. An age higher than 65 [odds ratio (OR) = 5.6, 95% confidence interval (CI): 2.2-14.4], the number of previous ablations (OR = 3.0, 95% CI: 1.2-7.8), and the management of ablation lines in the index procedure (OR = 2.5, 95% CI: 1.0-6.3) were independently associated with AFL occurrence. Furthermore, several characteristics assessed by LGE-CMR were identified as independent predictors of AFL recurrence after the index ablation for AF, such as enhanced LA sphericity (OR = 1.3, 95% CI: 1.1-1.6), LA global fibrosis (OR = 1.03, 95% CI: 1.01-1.07), and increased fibrosis in the lateral wall (OR = 1.03, 95% CI: 1.01-1.04).
Advanced atrial cardiomyopathy assessed by LGE-CMR, such as increased LA sphericity, global LA fibrosis, and fibrosis in the lateral wall, is independently associated with arrhythmia recurrence in the form of AFL following AF ablation.
在相当数量的患者中,房颤(AF)消融后出现非典型房性心动过速(AFL)形式的心律失常复发是很常见的,通常需要再次消融,但成功率有限。识别 AF 消融后发生 AFL 的高危患者有助于患者选择和个体化消融方法。本研究旨在评估预先存在的心房心肌病与 AF 消融后 AFL 发生之间的关系。
我们分析了连续 1007 例接受导管消融并纳入前瞻性登记的 AF 患者的队列。排除了基线无心脏磁共振成像和钆延迟增强(LGE-CMR)或无任何复发的患者。共纳入 166 例患者,其中 56 例因 AFL 复发而再次消融,110 例因 AF 复发而再次消融(P = 0.11)。基于 LGE-CMR 的心房心肌病的多参数评估包括左心房(LA)容积、LA 球形度以及使用半自动后处理软件的整体和节段性 LA 纤维化。在最初的 1007 例患者队列中,56 例患者出现 AFL,110 例患者出现 AF。年龄大于 65 岁(比值比 [OR] = 5.6,95%置信区间 [CI]:2.2-14.4)、既往消融次数(OR = 3.0,95% CI:1.2-7.8)和索引手术中消融线的管理(OR = 2.5,95% CI:1.0-6.3)与 AFL 发生独立相关。此外,通过 LGE-CMR 评估的几个特征被确定为 AF 消融后 AFL 复发的独立预测因素,例如增强的 LA 球形度(OR = 1.3,95% CI:1.1-1.6)、整体 LA 纤维化(OR = 1.03,95% CI:1.01-1.07)和外侧壁纤维化增加(OR = 1.03,95% CI:1.01-1.04)。
通过 LGE-CMR 评估的高级心房心肌病,如 LA 球形度增加、整体 LA 纤维化和外侧壁纤维化,与 AF 消融后 AFL 形式的心律失常复发独立相关。