Lancaster Medical School, Faculty of Health and Medicine, Health Innovation Campus, Lancaster University, Sir John Fisher Drive, Lancaster, Lancashire, LA1 4AT, UK.
Lancashire and South Cumbria NHS Foundation Trust, Sceptre Point, Sceptre Way, Bamber Bridge, Preston, Lancashire, PR5 6AW, UK.
BMC Health Serv Res. 2023 Sep 29;23(1):1042. doi: 10.1186/s12913-023-10030-8.
Population groups experience differential access to timely and high-quality mental healthcare. Despite efforts of recent UK policies to improve the accessibility of mental health services, there remains a lack of comprehensive understanding of inequalities in access to services needed to do this. This systematic mapping review aimed to address this gap by identifying which population groups continue to be poorly served by access to adult mental health services in the UK, how access has been measured, and what research methods have been applied.
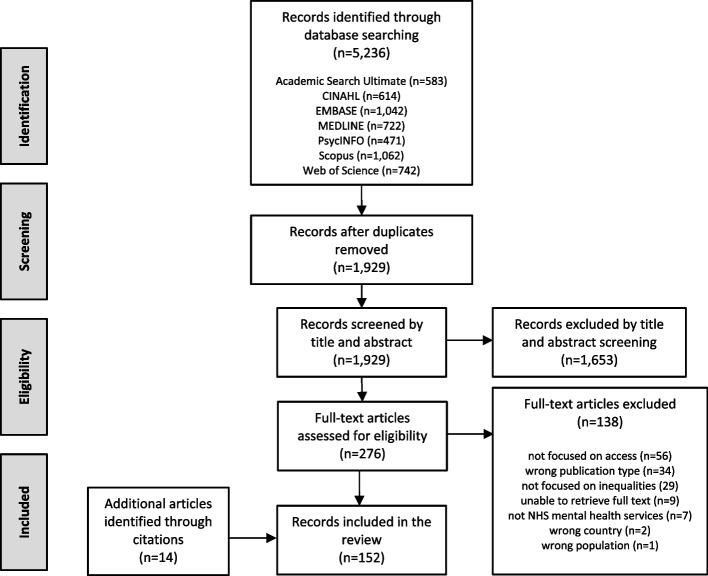
Seven electronic databases were searched from January 2014 up to May 2022. Primary research studies of any design were included if they examined access to adult NHS mental health services in the UK by population groups at risk of experiencing inequalities. Study characteristics, measures of access, inequalities studied, and key findings were extracted. A best-fit framework approach was used, applying Levesque's Conceptual Framework for Healthcare Access to synthesise measures of access, and applying a template derived from Cochrane Progress-Plus and NHS Long Term Plan equality characteristics to synthesise key findings associated with inequalities.
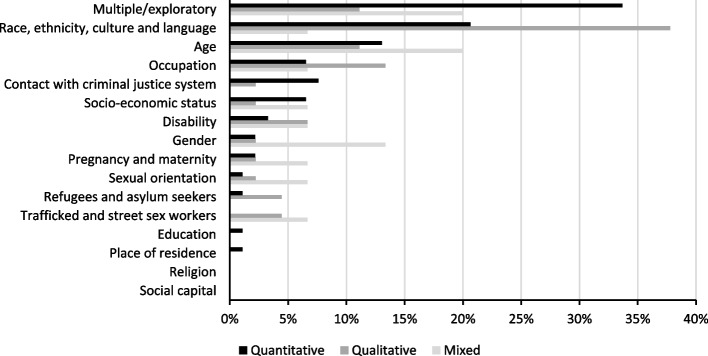
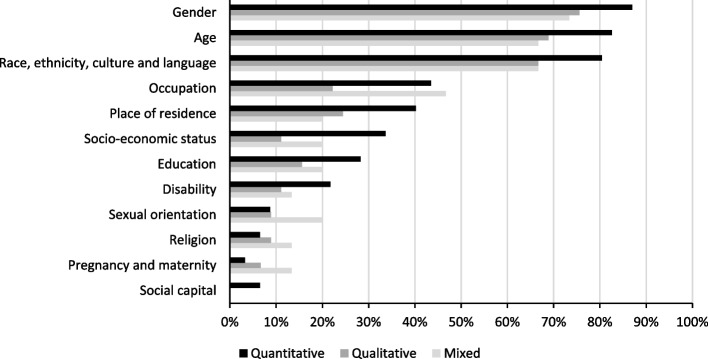
Of 1,929 publications retrieved, 152 studies of various types were included. The most frequently considered dimensions of inequality were gender, age, and ethnicity, whilst social capital, religion, and sexual orientation were least frequently considered. Most studies researched access by measuring "healthcare utilisation", followed by studies that measured "healthcare seeking". Key barriers to access were associated with individuals' "ability to seek" (e.g. stigma and discrimination) and "ability to reach" (e.g. availability of services). Almost half of the studies used routinely collected patient data, and only 16% of studies reported patient and public involvement.
Little appears to have changed in the nature and extent of inequalities, suggesting that mental health services have not become more accessible. Actions to reduce inequalities should address barriers to population groups' abilities to seek and reach services such as stigma-reducing interventions, and re-designing services and pathways. Significant benefits exist in using routinely collected patient data, but its limitations should not be ignored. More theoretically informed research, using a holistic measurement of access, is needed in this area.
不同人群获得及时和高质量精神卫生保健的机会存在差异。尽管英国最近的政策努力改善了精神卫生服务的可及性,但对于服务可及性方面的不平等问题仍缺乏全面的理解。本系统映射综述旨在通过确定哪些人群在获得英国成人精神卫生服务方面仍得不到充分服务,以及如何衡量服务的可及性,以及应用了哪些研究方法来解决这一差距。
从 2014 年 1 月到 2022 年 5 月,对七个电子数据库进行了搜索。如果研究通过有风险经历不平等的人群来检查英国国民保健制度精神卫生服务的可及性,那么任何设计的初级研究都包含在内。提取研究特征、可及性衡量标准、研究的不平等问题以及主要发现。应用 Levesque 的医疗保健可及性概念框架来综合可及性衡量标准,并应用源自 Cochrane Progress-Plus 和 NHS 长期计划平等特征的模板来综合与不平等相关的主要发现,采用最佳契合框架方法。
在检索到的 1929 篇出版物中,有 152 项不同类型的研究被纳入。最常考虑的不平等维度是性别、年龄和种族,而社会资本、宗教和性取向则很少被考虑。大多数研究通过衡量“医疗保健利用”来研究可及性,其次是衡量“寻求医疗保健”的研究。可及性的主要障碍与个人的“寻求能力”(例如,耻辱感和歧视)和“到达能力”(例如,服务的可获得性)有关。近一半的研究使用常规收集的患者数据,只有 16%的研究报告了患者和公众的参与。
不平等的性质和程度似乎没有什么变化,这表明精神卫生服务并没有变得更容易获得。减少不平等的行动应该解决阻碍人群寻求和到达服务的障碍,例如减少耻辱感的干预措施,以及重新设计服务和途径。在这一领域,使用常规收集的患者数据存在显著的好处,但不应忽视其局限性。需要在这一领域进行更多基于理论的研究,使用对可及性的全面衡量标准。