Department of General Surgery, Fondazione Poliambulanza Istituto Ospedaliero, Brescia, 25123, Italy.
Department of Surgery, Amsterdam UMC, location University of Amsterdam, Amsterdam, the Netherlands.
Trials. 2023 Oct 12;24(1):665. doi: 10.1186/s13063-023-07657-7.
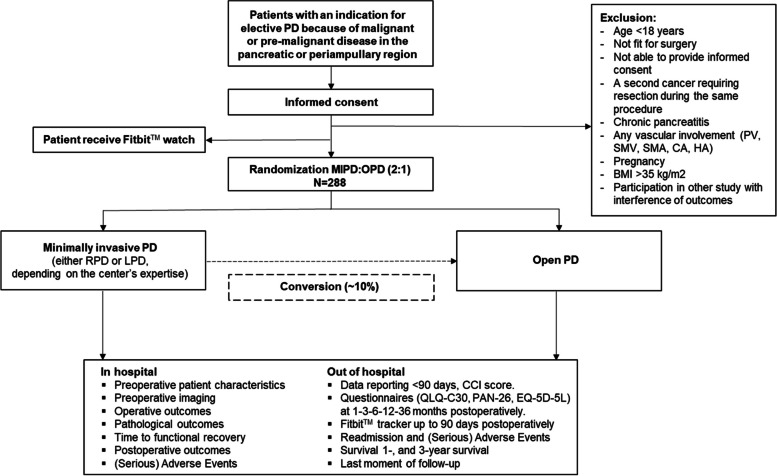
Minimally invasive pancreatoduodenectomy (MIPD) aims to reduce the negative impact of surgery as compared to open pancreatoduodenectomy (OPD) and is increasingly becoming part of clinical practice for selected patients worldwide. However, the safety of MIPD remains a topic of debate and the potential shorter time to functional recovery needs to be confirmed. To guide safe implementation of MIPD, large-scale international randomized trials comparing MIPD and OPD in experienced high-volume centers are needed. We hypothesize that MIPD is non-inferior in terms of overall complications, but superior regarding time to functional recovery, as compared to OPD.
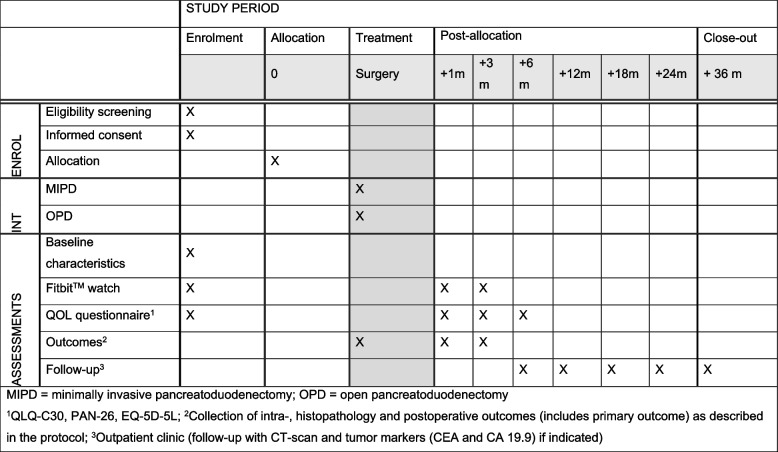
METHODS/DESIGN: The DIPLOMA-2 trial is an international randomized controlled, patient-blinded, non-inferiority trial performed in 14 high-volume pancreatic centers in Europe with a minimum annual volume of 30 MIPD and 30 OPD. A total of 288 patients with an indication for elective pancreatoduodenectomy for pre-malignant and malignant disease, eligible for both open and minimally invasive approach, are randomly allocated for MIPD or OPD in a 2:1 ratio. Centers perform either laparoscopic or robot-assisted MIPD based on their surgical expertise. The primary outcome is the Comprehensive Complication Index (CCI®), measuring all complications graded according to the Clavien-Dindo classification up to 90 days after surgery. The sample size is calculated with the following assumptions: 2.5% one-sided significance level (α), 80% power (1-β), expected difference of the mean CCI® score of 0 points between MIPD and OPD, and a non-inferiority margin of 7.5 points. The main secondary outcome is time to functional recovery, which will be analyzed for superiority. Other secondary outcomes include post-operative 90-day Fitbit™ measured activity, operative outcomes (e.g., blood loss, operative time, conversion to open surgery, surgeon-reported outcomes), oncological findings in case of malignancy (e.g., R0-resection rate, time to adjuvant treatment, survival), postoperative outcomes (e.g., clinically relevant complications), healthcare resource utilization (length of stay, readmissions, intensive care stay), quality of life, and costs. Postoperative follow-up is up to 36 months.
The DIPLOMA-2 trial aims to establish the safety of MIPD as the new standard of care for this selected patient population undergoing pancreatoduodenectomy in high-volume centers, ultimately aiming for superior patient recovery.
ISRCTN27483786. Registered on August 2, 2023.
微创胰十二指肠切除术(MIPD)旨在减轻手术对患者的负面影响,与开腹胰十二指肠切除术(OPD)相比,它在全球范围内越来越多地成为某些患者的临床选择。然而,MIPD 的安全性仍是一个争议话题,其潜在的功能恢复时间更短仍有待证实。为了安全实施 MIPD,需要在经验丰富的高容量中心进行大规模的国际随机试验,比较 MIPD 和 OPD。我们假设与 OPD 相比,MIPD 在总体并发症方面无差异,但在功能恢复时间方面更具优势。
方法/设计:DIPLOMA-2 试验是一项在欧洲 14 个高容量胰腺中心进行的国际随机对照、患者盲法、非劣效性试验,这些中心每年至少进行 30 例 MIPD 和 30 例 OPD。共有 288 例患有恶性和良性疾病的患者需要进行择期胰十二指肠切除术,这些患者适合开放和微创方法,按照 2:1 的比例随机分配接受 MIPD 或 OPD。中心根据手术专业知识进行腹腔镜或机器人辅助 MIPD。主要结局是综合并发症指数(CCI®),测量术后 90 天内根据 Clavien-Dindo 分级的所有并发症。根据以下假设计算样本量:单侧 2.5%显著性水平(α),80%功效(1-β),MIPD 和 OPD 之间预期 CCI®评分均值差值为 0 点,非劣效性边界为 7.5 点。主要次要结局是功能恢复时间,将分析其优越性。其他次要结局包括术后 90 天 Fitbit™测量的活动、手术结果(如出血量、手术时间、转为开腹手术、外科医生报告的结果)、恶性肿瘤的肿瘤学发现(如 R0 切除率、辅助治疗时间、生存率)、术后结果(如临床相关并发症)、医疗资源利用(住院时间、再入院、重症监护停留时间)、生活质量和成本。术后随访时间长达 36 个月。
DIPLOMA-2 试验旨在确定 MIPD 的安全性,作为高容量中心接受胰十二指肠切除术的这一选定患者群体的新护理标准,最终旨在实现患者更好的康复。
ISRCTN27483786。于 2023 年 8 月 2 日注册。