Certara Strategic Consulting, Paris, France.
Clinical Pharmacology, Genentech, South San Francisco, California, USA.
CPT Pharmacometrics Syst Pharmacol. 2024 Jan;13(1):68-78. doi: 10.1002/psp4.13057. Epub 2023 Oct 25.
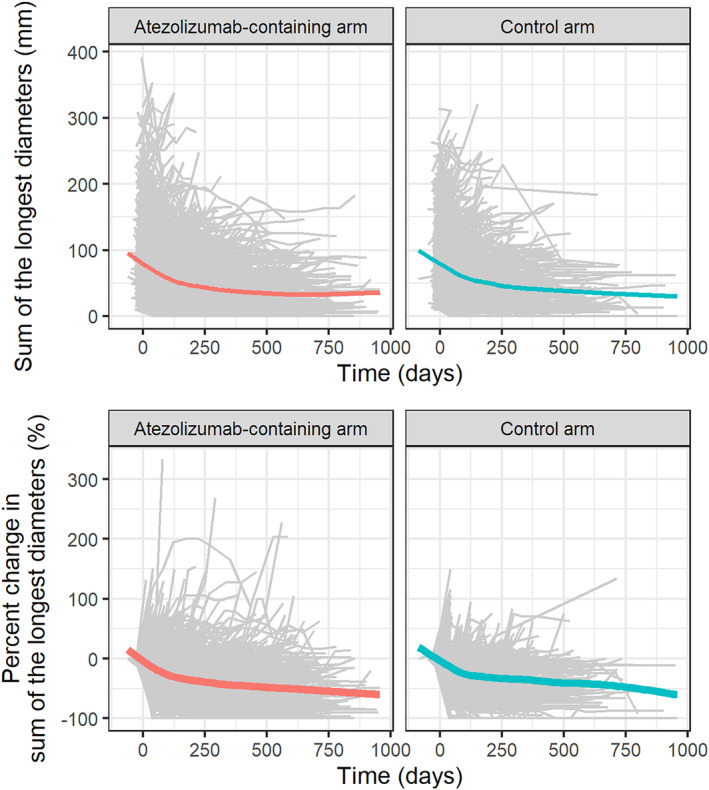
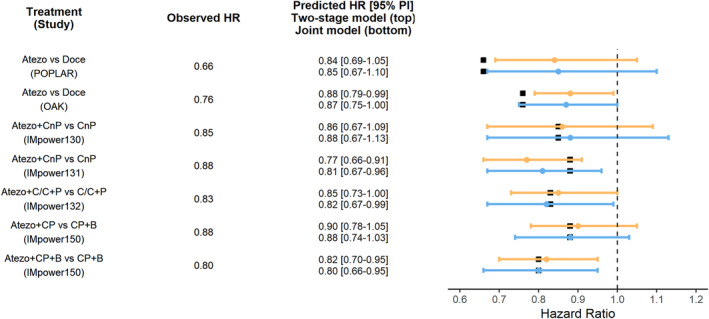
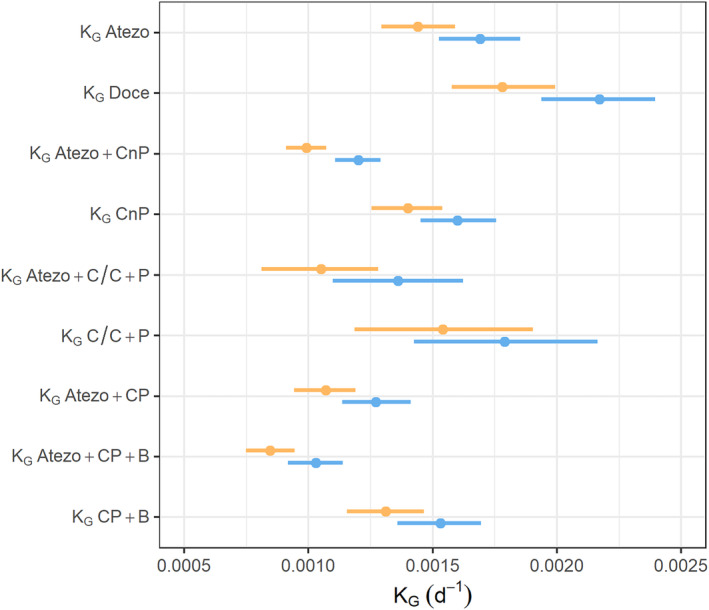
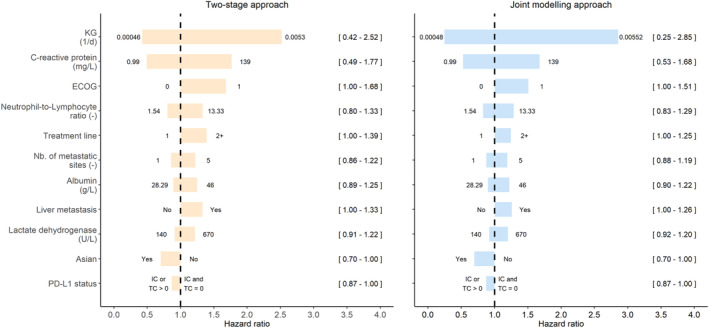
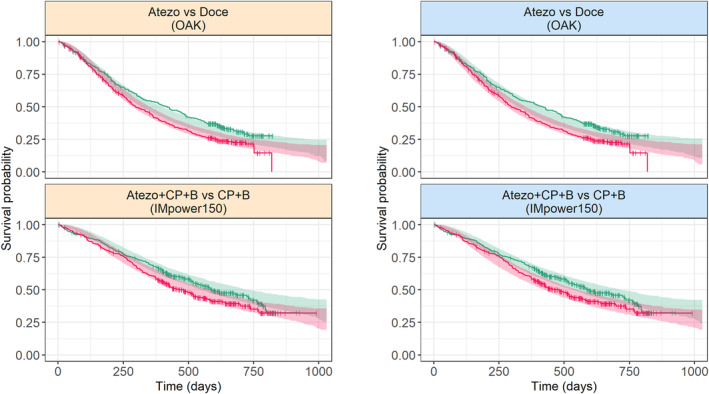
Two-stage and joint modeling approaches are the two main approaches to investigate the link between longitudinal tumor size data and overall survival (OS) and anticipate clinical trial outcome. We here used a large database composed of one phase II and five phase III clinical trials evaluating atezolizumab (an immunotherapy) in monotherapy or in combination with chemotherapies in 3699 patients with non-small cell lung cancer to evaluate the differences between both approaches in terms of parameter estimates, magnitude of covariate effects, and ability to predict OS. Although the two-stage approach may underestimate the magnitude of the impact of tumor growth rate (K ) on OS compared to joint modeling approach (hazard ratios [HRs] of 0.42-2.52 vs. 0.25-2.85, respectively, for individual K varying from the 5th and 95th percentiles), this difference did not lead into poorer performance of the two-stage approach to describe the OS distribution in the six clinical studies. Overall, two-stage and joint modeling approaches accurately predicted OS HR with a median (range) difference with the observed OS HR of 0.02 (0.01-0.18) and 0.03 (0.00-0.19), in all cases considered, respectively (e.g., for IMpower150: 0.80 [0.66-0.95] vs. 0.82 [0.70-0.95], respectively, whereas the observed OS HR was 0.80). In our setting, the two-stage approach accurately predicted the benefit of atezolizumab on OS. Further work is needed to verify if similar results are achieved using phase Ib or phase II clinical trials where the number of patients and measurements is limited as well as in other cancer indications.
两阶段和联合建模方法是研究纵向肿瘤大小数据与总生存期(OS)之间关系并预测临床试验结果的两种主要方法。我们使用了一个由一项 II 期和五项 III 期临床试验组成的大型数据库,这些试验评估了阿特珠单抗(一种免疫疗法)在非小细胞肺癌患者中的单药治疗或联合化疗治疗,共 3699 例患者,以评估两种方法在参数估计、协变量效应大小和预测 OS 能力方面的差异。虽然与联合建模方法相比,两阶段方法可能低估肿瘤生长率(K)对 OS 的影响程度(个体 K 从第 5 百分位到第 95 百分位变化时的风险比 [HR] 分别为 0.42-2.52 和 0.25-2.85),但这种差异并没有导致两阶段方法在描述六个临床试验中的 OS 分布方面表现不佳。总体而言,两阶段和联合建模方法准确地预测了 OS HR,与观察到的 OS HR 的中位数(范围)差异分别为 0.02(0.01-0.18)和 0.03(0.00-0.19),在所有情况下都得到了考虑(例如,对于 IMpower150:0.80[0.66-0.95]与 0.82[0.70-0.95],而观察到的 OS HR 为 0.80)。在我们的研究环境中,两阶段方法准确地预测了阿特珠单抗对 OS 的获益。需要进一步的工作来验证在患者和测量数量有限的 Ib 期或 II 期临床试验中以及在其他癌症适应症中是否也能获得类似的结果。