Department of Pediatric Oncology, Emma Childrens' Hospital UMC, Amsterdam, The Netherlands.
Department of Hematology-oncology, Princess Maxima Center for Pediatric Oncology, Utrecht, The Netherlands.
BMJ Open. 2023 Oct 29;13(10):e070804. doi: 10.1136/bmjopen-2022-070804.
Health-related quality of life (HRQoL) is impaired in paediatric patients with acute lymphoblastic leukaemia (ALL). Over the past decades, ALL treatment has successfully been adjusted to the risk of relapse, which is now reflected by the stratification of patients into three risk groups who receive treatment of differing intensities. This study is the first to evaluate the longitudinal course of HRQoL in light of these adjustments and identify determinants of HRQoL.
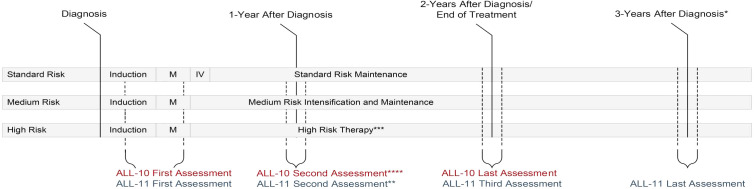
Two prospective, national cohort studies (add-on studies within the two most recent treatment protocols for children with ALL (ALL-10 and ALL-11)).
Dutch paediatric oncology hospitals between October 2006 and October 2009 (ALL-10) and between August 2013 and July 2017 (ALL-11).
Patients with ALL (2-18 years) are treated according to the ALL-10 or ALL-11 treatment protocol. Patients treated according to the ALL-10 protocol only completed a cancer-specific QoL measure and patients treated according to the ALL-11 protocol completed both a cancer-specific and generic QoL measure (see below).
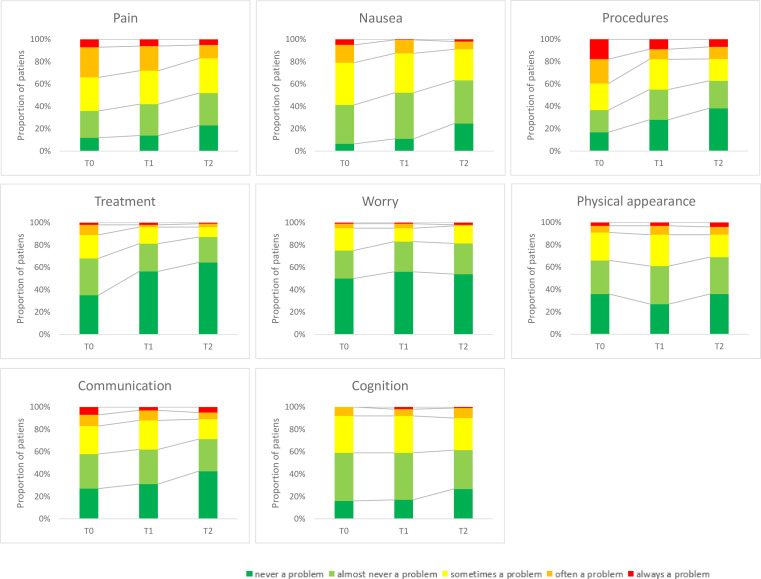
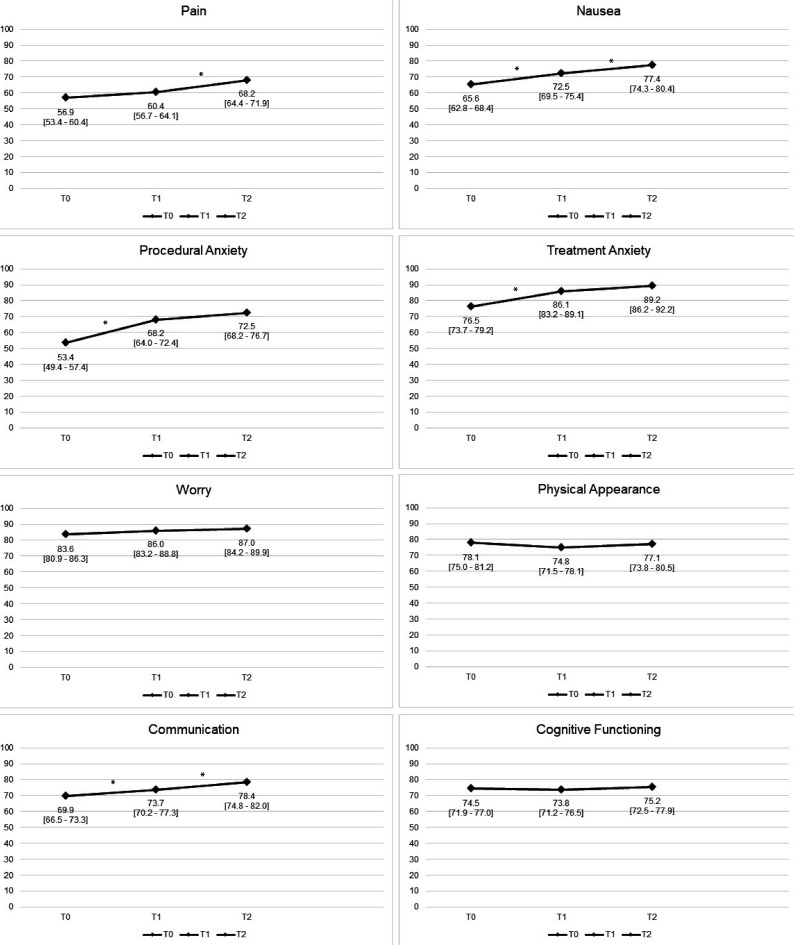
HRQoL, assessed with parent-proxy questionnaires (PedsQL Generic and Cancer module) within the first 5 months (T0), at 1 year (T1), 2 years (T2) and 3 years (T3) after diagnosis. The proportion of patients with clinically relevant generic HRQoL impairment was compared with healthy norm values. Multivariable mixed model analyses were used to evaluate the development of HRQoL over time and its medical and sociodemographic determinants (collected on enrolment).
Of the ALL-10 cohort, 132 families participated and of the ALL-11 cohort, 136 families participated (268 total). Thus, cancer-specific HRQoL assessments were available for 268 patients (median age 5.3 years (IQR 6.15), 56.0% boys, 69.0% medium-risk ALL), and generic HRQoL assessments for 136 patients (median age 4.8 years (IQR 6.13), 60.3% boys, 75.0% medium-risk ALL). Generic HRQoL improved between timepoints T0 and T3 (total score B 16.1, 95% CI 12.2 to 20.1, p<0.001), but did not restore to normal 1 year after the end of treatment: 28.0% of children remained impaired compared with 16% in the general population (p=0.003). Cancer-specific HRQoL generally improved from T0 to T2 (Pain B 11.3, 95% CI 7.1 to 15.5; Nausea B 11.7, 8.4 to 15.1; Procedural Anxiety B 19.1, 14.8 to 23.4; Treatment Anxiety B 12.8, 9.5 to 16.0; Worry B 3.5, 0.6 to 6.3; Communication B 8.5, 5.0 to 11.9; all p<0.001 except for Worry (p=0.02)), while Physical Appearance and Cognitive Functioning remained stable. Higher treatment intensity and experiencing pain or simultaneous chronic illness were associated with lower HRQoL over time for multiple subscales.
HRQoL impairment is prevalent during and after ALL treatment. Patients with standard-risk ALL and reduced treatment intensity have better HRQoL than patients in higher risk groups. Systematic monitoring of HRQoL is of utmost importance in order to provide timely psychosocial interventions and supportive care.
儿童急性淋巴细胞白血病(ALL)患者的健康相关生活质量(HRQoL)受损。在过去的几十年中,ALL 的治疗已成功地根据复发风险进行了调整,现在通过将患者分为接受不同强度治疗的三个风险组来反映这种调整。这项研究首次根据这些调整评估了 HRQoL 的纵向过程,并确定了 HRQoL 的决定因素。
两项前瞻性、全国性队列研究(ALL-10 和 ALL-11 两个最新儿童 ALL 治疗方案中的附加研究)。
2006 年 10 月至 2009 年 10 月(ALL-10)和 2013 年 8 月至 2017 年 7 月(ALL-11)荷兰儿科肿瘤医院。
根据 ALL-10 或 ALL-11 治疗方案治疗的 ALL 患者(2-18 岁)。仅根据 ALL-10 方案治疗的患者完成了癌症特异性 QoL 测量,而根据 ALL-11 方案治疗的患者完成了癌症特异性和通用 QoL 测量(见下文)。
HRQoL,使用父母代理问卷(PedsQL 通用和癌症模块)在诊断后的前 5 个月(T0)、1 年(T1)、2 年(T2)和 3 年(T3)评估。将患有临床相关通用 HRQoL 损害的患者比例与健康标准值进行比较。使用多变量混合模型分析评估 HRQoL 的随时间发展及其医疗和社会人口统计学决定因素(在入组时收集)。
ALL-10 队列中,132 个家庭参与,ALL-11 队列中,136 个家庭参与(共 268 个)。因此,268 名患者提供了癌症特异性 HRQoL 评估(中位年龄 5.3 岁(IQR 6.15),56.0%为男孩,69.0%为中危 ALL),136 名患者提供了通用 HRQoL 评估(中位年龄 4.8 岁(IQR 6.13),60.3%为男孩,75.0%为中危 ALL)。通用 HRQoL 在 T0 至 T3 之间有所改善(总分 B 16.1,95%CI 12.2 至 20.1,p<0.001),但治疗结束后 1 年仍未恢复正常:与普通人群中的 16%相比,仍有 28.0%的儿童存在受损(p=0.003)。癌症特异性 HRQoL 通常从 T0 到 T2 有所改善(疼痛 B 11.3,95%CI 7.1 至 15.5;恶心 B 11.7,8.4 至 15.1;程序焦虑 B 19.1,14.8 至 23.4;治疗焦虑 B 12.8,9.5 至 16.0;担心 B 3.5,0.6 至 6.3;沟通 B 8.5,5.0 至 11.9;所有 p<0.001,除了担心(p=0.02)),而身体外观和认知功能保持稳定。较高的治疗强度和经历疼痛或同时患有慢性疾病与多个子量表的 HRQoL 随时间下降有关。
ALL 治疗期间和治疗后,HRQoL 受损普遍存在。标准风险 ALL 患者和降低治疗强度的患者的 HRQoL 优于高危组患者。系统监测 HRQoL 对于及时提供心理社会干预和支持性护理至关重要。