Department of Medical Biotechnology, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
Department of Production Platforms & Analytics, Human Health Therapeutics Research Centre, National Research Council Canada, Montreal, QC, Canada.
Front Immunol. 2023 Dec 7;14:1302307. doi: 10.3389/fimmu.2023.1302307. eCollection 2023.
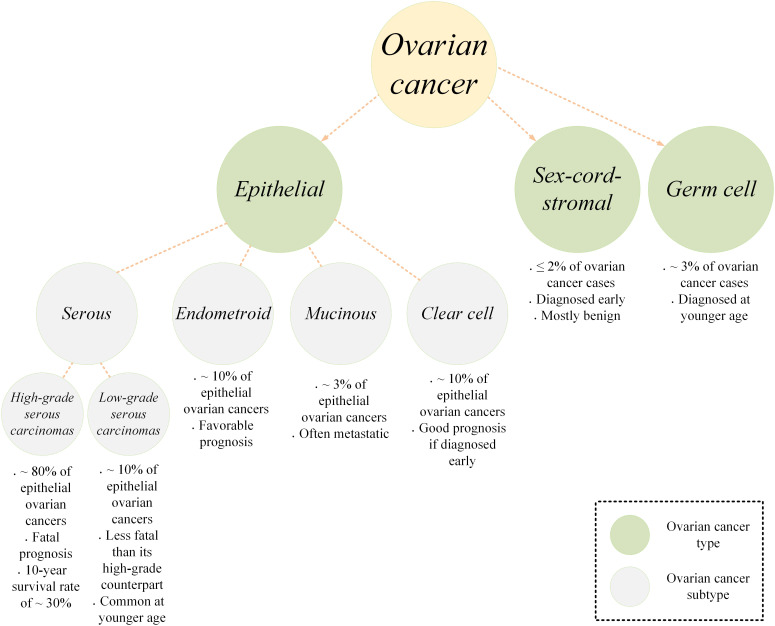
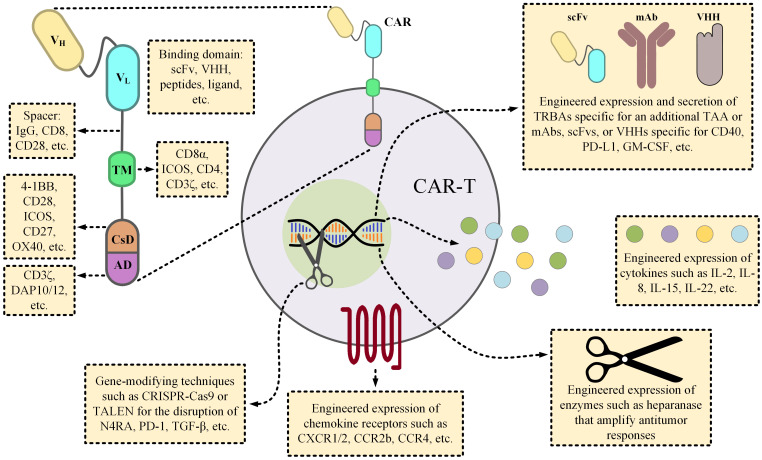
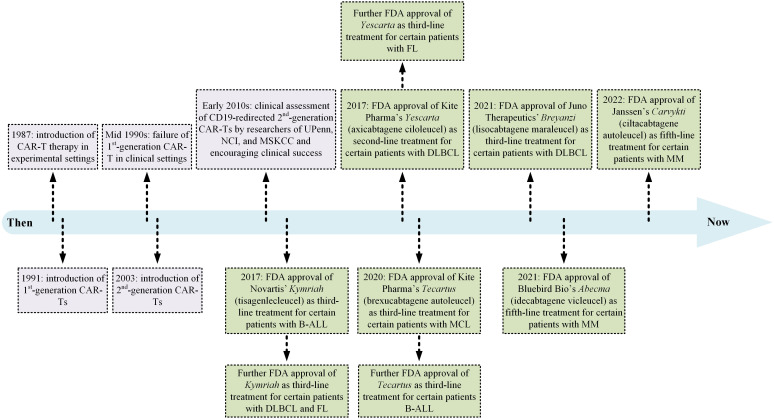
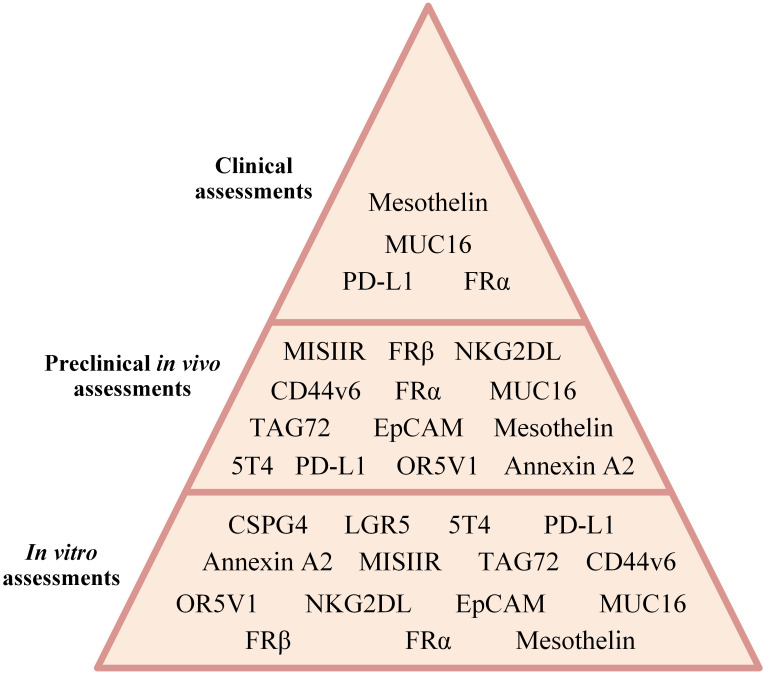
As the most lethal gynecologic oncological indication, carcinoma of the ovary has been ranked as the 5 cause of cancer-related mortality in women, with a high percentage of the patients being diagnosed at late stages of the disease and a five-year survival of ~ 30%. Ovarian cancer patients conventionally undergo surgery for tumor removal followed by platinum- or taxane-based chemotherapy; however, a high percentage of patients experience tumor relapse. Cancer immunotherapy has been regarded as a silver lining in the treatment of patients with various immunological or oncological indications; however, mirvetuximab soravtansine (a folate receptor α-specific mAb) and bevacizumab (a VEGF-A-specific mAb) are the only immunotherapeutics approved for the treatment of ovarian cancer patients. Chimeric antigen receptor T-cell (CAR-T) therapy has achieved tremendous clinical success in the treatment of patients with certain B-cell lymphomas and leukemias, as well as multiple myeloma. In the context of solid tumors, CAR-T therapies face serious obstacles that limit their therapeutic benefit. Such hindrances include the immunosuppressive nature of solid tumors, impaired tumor infiltration, lack of qualified tumor-associated antigens, and compromised stimulation and persistence of CAR-Ts following administration. Over the past years, researchers have made arduous attempts to apply CAR-T therapy to ovarian cancer. In this review, we outline the principles of CAR-T therapy and then highlight its limitations in the context of solid tumors. Ultimately, we focus on preclinical and clinical findings achieved in CAR-T-mediated targeting of different ovarian cancer-associated target antigens.
作为最致命的妇科肿瘤学指征,卵巢癌已成为女性癌症相关死亡的第 5 大原因,大多数患者在疾病晚期被诊断出来,五年生存率约为 30%。卵巢癌患者通常接受手术切除肿瘤,然后进行铂类或紫杉烷类化疗;然而,大多数患者会经历肿瘤复发。癌症免疫疗法被认为是治疗各种免疫或肿瘤学指征患者的一线希望;然而,mirvetuximab soravtansine(一种叶酸受体 α 特异性 mAb)和贝伐单抗(一种 VEGF-A 特异性 mAb)是唯一批准用于治疗卵巢癌患者的免疫疗法。嵌合抗原受体 T 细胞(CAR-T)疗法在治疗某些 B 细胞淋巴瘤和白血病以及多发性骨髓瘤方面取得了巨大的临床成功。在实体肿瘤方面,CAR-T 疗法面临着严重的障碍,限制了其治疗效果。这些障碍包括实体肿瘤的免疫抑制性质、肿瘤浸润受损、缺乏合格的肿瘤相关抗原,以及 CAR-T 给药后的刺激和持续存在受损。在过去的几年中,研究人员一直在努力将 CAR-T 疗法应用于卵巢癌。在这篇综述中,我们概述了 CAR-T 疗法的原理,然后强调了其在实体肿瘤中的局限性。最终,我们将重点放在 CAR-T 介导的针对不同卵巢癌相关靶抗原的靶向的临床前和临床研究结果上。