Department of Neurosurgery, Division of Spine Surgery, Technische Universität Dresden, Faculty of Medicine, and University Hospital Carl Gustav Carus, Fetscherstrasse 74, 01307, Dresden, Germany.
Department of Neurology, Technische Universität Dresden, Faculty of Medicine, and University Hospital Carl Gustav Carus, Fetscherstrasse 74, 01307, Dresden, Germany.
BMC Infect Dis. 2024 Jan 2;24(1):39. doi: 10.1186/s12879-023-08946-x.
Personalized clinical management of spondylodiscitis (SD) and isolated spinal epidural empyema (ISEE) is challenging due to limited evidence of microbiologic findings and their clinical impact during the clinical course of the disease. We aimed to characterize clinico-microbiological and imaging phenotypes of SD and ISEE to provide useful insights that could improve outcomes and potentially modify guidelines.
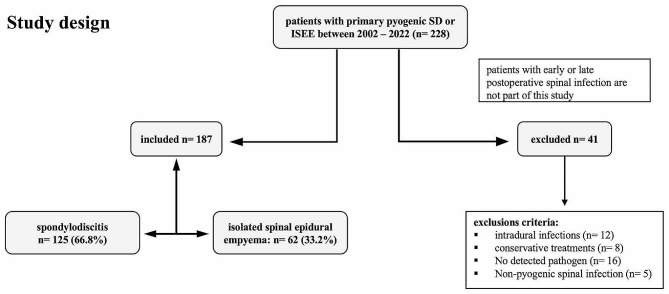
We performed chart review and collected data on the following parameters: bacterial antibiogram-resistogram, type of primary spinal infection, location of spinal infection, source of infection, method of detection, clinical complications (sepsis, septic embolism, and endocarditis), length of hospital and intensive care unit (ICU) stay, relapse rate, and disease-related mortality in patients with proven pyogenic SD and ISEE treated surgically in a university hospital in Germany between 2002 and 2022.
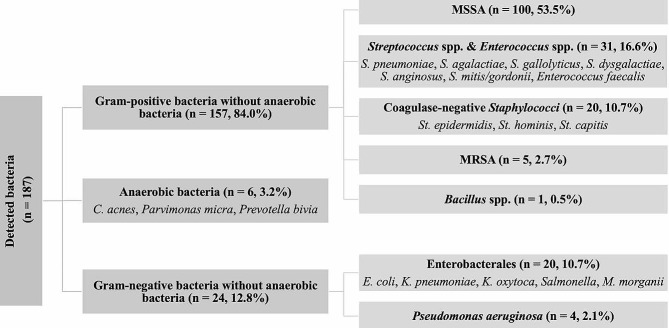
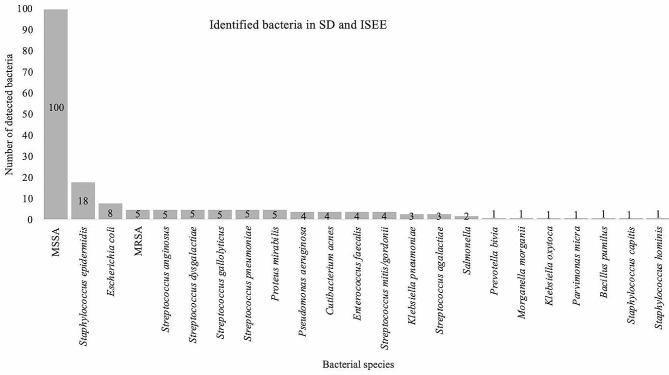
We included data from 187 patients (125 SD, 66.8% and 62 ISEE, 33.2%). Gram-positive bacteria (GPB) were overall more frequently detected than gram-negative bacteria (GNB) (GPB: 162, 86.6% vs. GNB: 25, 13.4%, p < 0.001). Infective endocarditis was caused only by GPB (GPB: 23, 16.5% vs. GNB: 0, 0.0%, p = 0.046). Methicillin-susceptible Staphylococcus aureus was the most frequently isolated strain (MSSA: n = 100, 53.5%), occurred more frequently in the cervical spine compared to other bacteria (OB) (MSSA: 41, 41.0% vs. OB: 18, 20.7%, p = 0.004) and was most frequently detected in patients with skin infection as the primary source of infection (MSSA: 26, 40.6% vs. OB: 11, 16.7%, p = 0.002). Streptococcus spp. and Enterococcus spp. (SE: n = 31, 16.6%) were more often regarded as the cause of endocarditis (SE: 8, 27.6% vs. OB: 15, 11.4%, p = 0.037) and were less frequently detected in intraoperative specimens (SE: 19, 61.3% vs. OB: 138, 88.5%, p < 0.001). Enterobacterales (E: n = 20, 10.7%) were identified more frequently in urinary tract infections (E: 9, 50.0% vs. OB: 4, 3.6%, p < 0.001). Coagulase-negative Staphylococci (CoNS: n = 20, 10.7%) were characterized by a lower prevalence of sepsis (CoNS: 4, 20.0% vs. OB: 90, 53.9%, p = 0.004) and were more frequently detected in intraoperative specimens (CoNS: 20, 100. 0% vs. OB: 137, 82.0%, p = 0.048). Moreover, CoNS-associated cases showed a shorter length of ICU stay (CoNS: 2 [1-18] days vs. OB: 6 [1-53] days, median [interquartile range], p = 0.037), and occurred more frequently due to foreign body-associated infections (CoNS: 8, 61.5% vs. OB: 15, 12.8%, p = 0.008). The presence of methicillin-resistant Staphylococcus aureus (MRSA) prolonged hospital stay by 56 [24-58] days and ICU stay by 16 [1-44] days, whereas patients with Pseudomonas aeruginosa spent only 20 [18-29] days in the hospital and no day in the ICU 0 [0-5] days.
Our retrospective cohort study identified distinct bacterial-specific manifestations in pyogenic SD and ISEE regarding clinical course, neuroanatomic targets, method of pathogen detection, and sources of infection. The clinico-microbiological patterns varied depending on the specific pathogens.
由于疾病过程中微生物学发现及其临床影响的有限证据,脊柱骨髓炎(SD)和孤立性脊髓硬膜外脓肿(ISEE)的个性化临床管理具有挑战性。我们旨在描述 SD 和 ISEE 的临床微生物学和影像学表型,以提供有用的见解,从而改善结果并可能修改指南。
我们进行了病历回顾,并收集了以下参数的数据:细菌抗生素耐药谱、原发性脊柱感染类型、脊柱感染部位、感染源、检测方法、临床并发症(败血症、败血症栓子和心内膜炎)、住院和重症监护病房(ICU)住院时间、复发率和疾病相关死亡率。在德国的一所大学医院,对接受手术治疗的明确化脓性 SD 和 ISEE 患者进行了回顾性队列研究,研究时间为 2002 年至 2022 年。
我们纳入了 187 名患者的数据(125 例 SD,占 66.8%;62 例 ISEE,占 33.2%)。革兰氏阳性菌(GPB)的检出率明显高于革兰氏阴性菌(GNB)(GPB:162 例,占 86.6%;GNB:25 例,占 13.4%,p<0.001)。感染性心内膜炎仅由 GPB 引起(GPB:23 例,占 16.5%;GNB:0 例,占 0.0%,p=0.046)。甲氧西林敏感金黄色葡萄球菌(MSSA)是最常分离的菌株(n=100,占 53.5%),与其他细菌(OB)相比,更常发生在颈椎(MSSA:41 例,占 41.0%;OB:18 例,占 20.7%,p=0.004),并且最常从皮肤感染的原发灶中检测到(MSSA:26 例,占 40.6%;OB:11 例,占 16.7%,p=0.002)。链球菌属和肠球菌属(SE)(n=31,占 16.6%)更常被认为是心内膜炎的病因(SE:8 例,占 27.6%;OB:15 例,占 11.4%,p=0.037),并且在术中标本中较少被检出(SE:19 例,占 61.3%;OB:138 例,占 88.5%,p<0.001)。肠杆菌科(E)(n=20,占 10.7%)更常从尿路感染中检出(E:9 例,占 50.0%;OB:4 例,占 3.6%,p<0.001)。凝固酶阴性葡萄球菌(CoNS)(n=20,占 10.7%)的败血症发生率较低(CoNS:4 例,占 20.0%;OB:90 例,占 53.9%,p=0.004),并且更常从术中标本中检出(CoNS:20 例,占 100.0%;OB:137 例,占 82.0%,p=0.048)。此外,CoNS 相关病例的 ICU 住院时间更短(CoNS:2[1-18]天;OB:6[1-53]天,中位数[四分位间距],p=0.037),并且更常因异物相关感染引起(CoNS:8 例,占 61.5%;OB:15 例,占 12.8%,p=0.008)。耐甲氧西林金黄色葡萄球菌(MRSA)的存在使住院时间延长了 56[24-58]天,ICU 住院时间延长了 16[1-44]天,而铜绿假单胞菌感染的患者住院时间仅为 20[18-29]天,无 ICU 住院时间(0[0-5]天)。
我们的回顾性队列研究在化脓性 SD 和 ISEE 中确定了不同的细菌特异性表现,涉及临床病程、神经解剖学靶标、病原体检测方法和感染源。临床微生物学模式取决于特定的病原体。