Division of Pediatrics and Neonatal Critical Care, "A.Béclère" Medical Center, Paris- Saclay University Hospitals, APHP, Paris, France.
Physiopathology and Therapeutic Innovation Unit-INSERM U999, Paris-Saclay University, Paris, France.
Respir Res. 2024 Jan 4;25(1):12. doi: 10.1186/s12931-023-02651-8.
There are relatively few data about the ultrasound evaluation of pleural line in patients with respiratory failure. We measured the pleural line thickness during different phases of the respiratory cycle in neonates with and without acute respiratory failure as we hypothesized that this can significantly change.
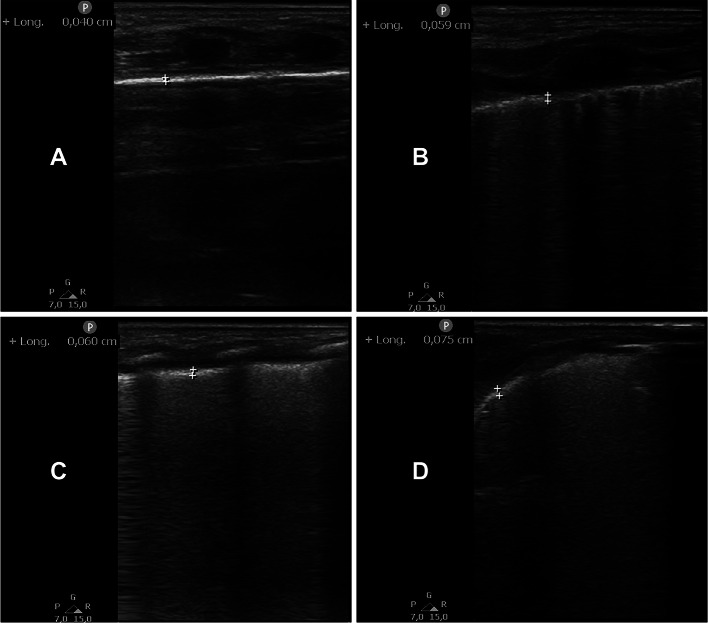
Prospective, observational, cohort study performed in an academic tertiary neonatal intensive care unit recruiting neonates with transient tachypnoea of the neonate (TTN), respiratory distress syndrome (RDS) or neonatal acute respiratory distress syndrome (NARDS). Neonates with no lung disease (NLD) were also recruited as controls. Pleural line thickness was measured with high-frequency ultrasound at end-inspiration and end-expiration by two different raters.
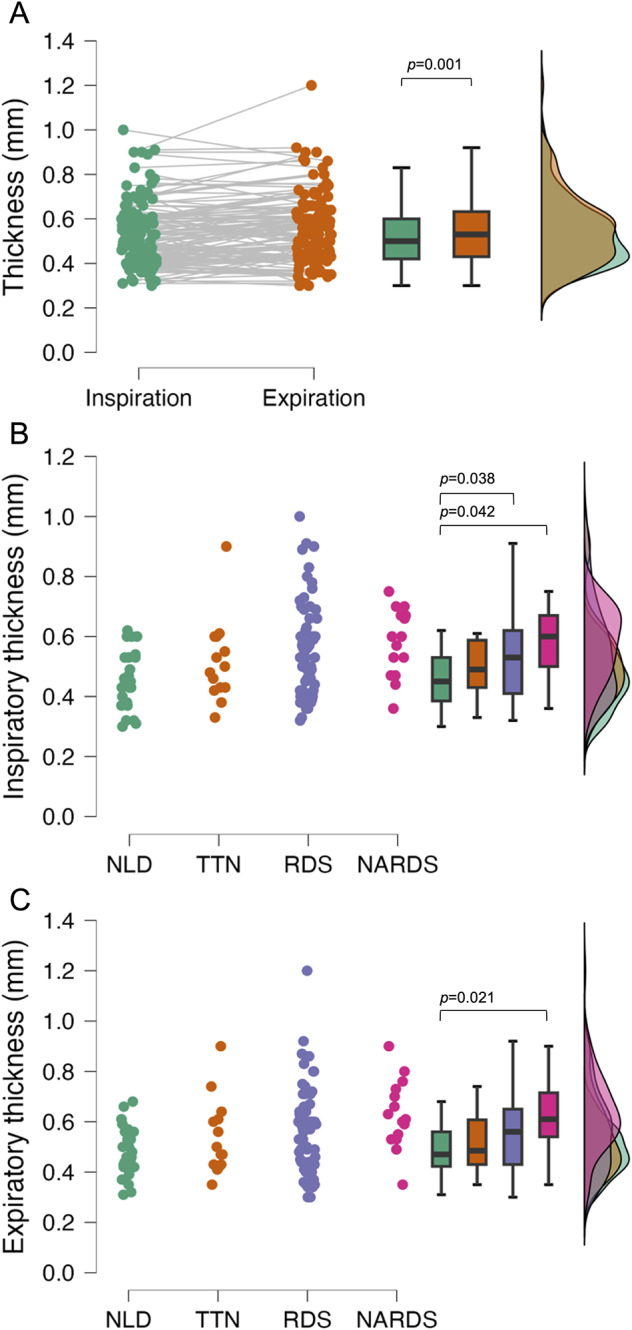
Pleural line thickness was slightly but significantly higher at end-expiration (0.53 [0.43-0.63] mm) than at end-inspiration (0.5 [0.4-0.6] mm; p = 0.001) for the whole population. End-inspiratory (NLD: 0.45 [0.38-0.53], TTN: 0.49 [0.43-0.59], RDS: 0.53 [0.41-0.62], NARDS: 0.6 [0.5-0.7] mm) and -expiratory (NLD: 0.47 [0.42-0.56], TTN: 0.48 [0.43-0.61], RDS: 0.53 [0.46-0.65], NARDS: 0.61 [0.54-0.72] mm) thickness were significantly different (overall p = 0.021 for both), between the groups although the absolute differences were small. The inter-rater agreement was optimal (ICC: 0.95 (0.94-0.96)). Coefficient of variation was 2.8% and 2.5% for end-inspiratory and end-expiratory measurements, respectively. These findings provide normative data of pleural line thickness for the most common forms of neonatal acute respiratory failure and are useful to design future studies to investigate possible clinical applications.
关于呼吸衰竭患者胸膜线的超声评估,相关数据相对较少。我们假设在呼吸周期的不同阶段,胸膜线厚度会发生显著变化,因此测量了伴有和不伴有急性呼吸衰竭的新生儿的胸膜线厚度。还招募了无肺部疾病(NLD)的新生儿作为对照。通过两名不同的评估者,在吸气末和呼气末使用高频超声测量胸膜线厚度。
这是一项在学术性三级新生儿重症监护病房进行的前瞻性、观察性队列研究,招募了患有新生儿暂时性呼吸急促(TTN)、呼吸窘迫综合征(RDS)或新生儿急性呼吸窘迫综合征(NARDS)的新生儿。还招募了无肺部疾病(NLD)的新生儿作为对照。通过两名不同的评估者,在吸气末和呼气末使用高频超声测量胸膜线厚度。
整个研究人群中,胸膜线厚度在呼气末(0.53[0.43-0.63]mm)略高于吸气末(0.5[0.4-0.6]mm;p=0.001)。吸气末(NLD:0.45[0.38-0.53]mm,TTN:0.49[0.43-0.59]mm,RDS:0.53[0.41-0.62]mm,NARDS:0.6[0.5-0.7]mm)和呼气末(NLD:0.47[0.42-0.56]mm,TTN:0.48[0.43-0.61]mm,RDS:0.53[0.46-0.65]mm,NARDS:0.61[0.54-0.72]mm)胸膜线厚度存在显著差异(两组间总体差异有统计学意义,p=0.021),但绝对差异较小。两名评估者间的一致性极佳(ICC:0.95(0.94-0.96))。吸气末和呼气末测量的变异系数分别为 2.8%和 2.5%。这些发现为最常见形式的新生儿急性呼吸衰竭的胸膜线厚度提供了正常参考数据,有助于设计未来的研究来探索可能的临床应用。