Stern Casey M, McPherson Iman, Dreier Melissa J, Coniglio Kathryn, Palmer Lilian P, Gydus Julia, Graver Haley, Germine Laura T, Tabri Nassim, Wang Shirley B, Breithaupt Lauren, Eddy Kamryn T, Thomas Jennifer J, Plessow Franziska, Becker Kendra R
Eating Disorders Clinical and Research Program, Massachusetts General Hospital, 2 Longfellow Place, Suite 200, Boston, MA, 02114, USA.
Neuroendocrine Unit, Massachusetts General Hospital, Boston, USA.
J Eat Disord. 2024 Jan 29;12(1):19. doi: 10.1186/s40337-023-00958-x.
Avoidant/restrictive food intake disorder (ARFID) and anorexia nervosa (AN) are the two primary restrictive eating disorders; however, they are driven by differing motives for inadequate dietary intake. Despite overlap in restrictive eating behaviors and subsequent malnutrition, it remains unknown if ARFID and AN also share commonalities in their cognitive profiles, with cognitive alterations being a key identifier of AN. Discounting the present value of future outcomes with increasing delay to their expected receipt represents a core cognitive process guiding human decision-making. A hallmark cognitive characteristic of individuals with AN (vs. healthy controls [HC]) is reduced discounting of future outcomes, resulting in reduced impulsivity and higher likelihood of favoring delayed gratification. Whether individuals with ARFID display a similar reduction in delay discounting as those with AN (vs. an opposing bias towards increased delay discounting or no bias) is important in informing transdiagnostic versus disorder-specific cognitive characteristics and optimizing future intervention strategies.
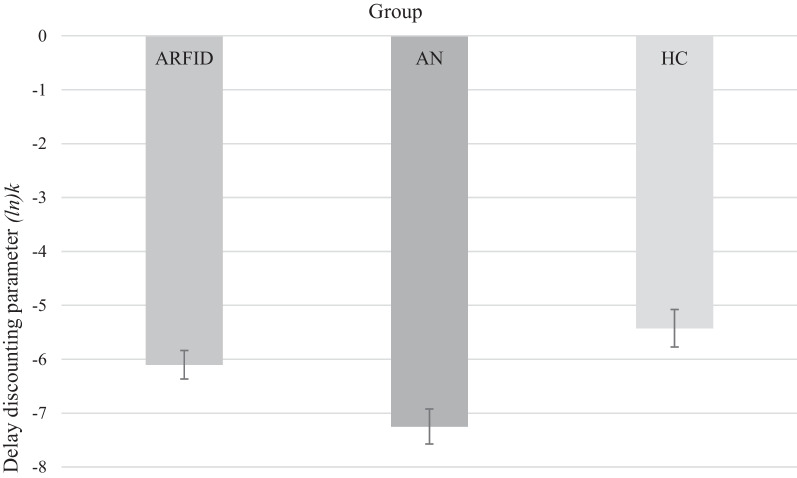
To address this research question, 104 participants (ARFID: n = 57, AN: n = 28, HC: n = 19) completed a computerized Delay Discounting Task. Groups were compared by their delay discounting parameter (ln)k.
Individuals with ARFID displayed a larger delay discounting parameter than those with AN, indicating steeper delay discounting (M ± SD = -6.10 ± 2.00 vs. -7.26 ± 1.73, p = 0.026 [age-adjusted], Hedges' g = 0.59), with no difference from HC (p = 0.514, Hedges' g = -0.35).
Our findings provide a first indication of distinct cognitive profiles among the two primary restrictive eating disorders. The present results, together with future research spanning additional cognitive domains and including larger and more diverse samples of individuals with ARFID (vs. AN), will contribute to identifying maintenance mechanisms that are unique to each disorder as well as contribute to the optimization and tailoring of treatment strategies across the spectrum of restrictive eating disorders.
回避/限制性食物摄入障碍(ARFID)和神经性厌食症(AN)是两种主要的限制性饮食障碍;然而,它们饮食摄入不足的动机不同。尽管在限制性饮食行为和随后的营养不良方面存在重叠,但ARFID和AN在认知特征上是否也有共同之处仍不清楚,而认知改变是AN的一个关键特征。随着预期获得未来结果的延迟增加,低估其现值是指导人类决策的核心认知过程。AN患者(与健康对照者[HC]相比)的一个标志性认知特征是对未来结果的折扣减少,从而导致冲动性降低,更有可能倾向于延迟满足。ARFID患者是否表现出与AN患者类似的延迟折扣减少(与对延迟折扣增加的相反偏差或无偏差相比),对于了解跨诊断与特定障碍的认知特征以及优化未来干预策略很重要。
为了解决这个研究问题,104名参与者(ARFID组:n = 57,AN组:n = 28,HC组:n = 19)完成了一项计算机化延迟折扣任务。通过延迟折扣参数(ln)k对各组进行比较。
ARFID患者的延迟折扣参数大于AN患者,表明延迟折扣更陡峭(M±SD = -6.10±2.00 vs. -7.26±1.73,p = 0.026[年龄调整后],Hedges' g = 0.59),与HC组无差异(p = 0.514,Hedges' g = -0.35)。
我们的研究结果首次表明了两种主要的限制性饮食障碍之间存在不同的认知特征。目前的结果,以及未来跨越更多认知领域并纳入更大、更多样化的ARFID(与AN相比)个体样本的研究,将有助于识别每种障碍特有的维持机制,并有助于优化和调整整个限制性饮食障碍范围内的治疗策略。