Department of Neurosurgery, Heidelberg University Hospital, Im Neuenheimer Feld 400, 69120, Heidelberg, Germany.
Department of Neurosurgery, Medical Faculty, Heidelberg University, Heidelberg, Germany.
J Neurooncol. 2024 Apr;167(2):245-255. doi: 10.1007/s11060-024-04595-5. Epub 2024 Feb 9.
Surgery for recurrent glioma provides cytoreduction and tissue for molecularly informed treatment. With mostly heavily pretreated patients involved, it is unclear whether the benefits of repeat surgery outweigh its potential risks.
Patients receiving surgery for recurrent glioma WHO grade 2-4 with the goal of tissue sampling for targeted therapies were analyzed retrospectively. Complication rates (surgical, neurological) were compared to our institutional glioma surgery cohort. Tissue molecular diagnostic yield, targeted therapies and post-surgical survival rates were analyzed.
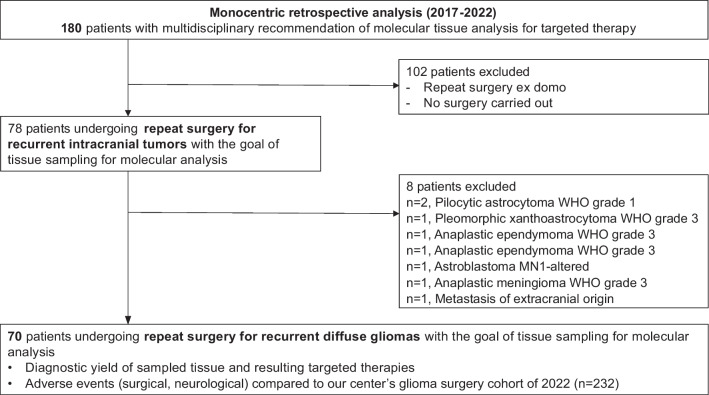
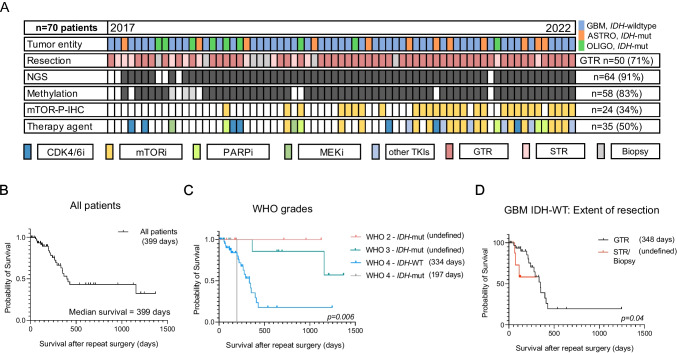
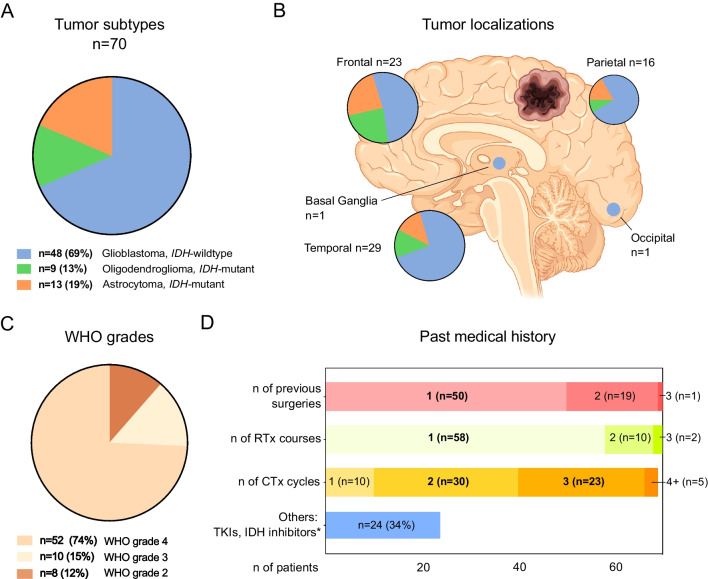
Between 2017 and 2022, tumor board recommendation for targeted therapy through molecular diagnostics was made for 180 patients. Of these, 70 patients (38%) underwent repeat surgery. IDH-wildtype glioblastoma was diagnosed in 48 patients (69%), followed by IDH-mutant astrocytoma (n = 13; 19%) and oligodendroglioma (n = 9; 13%). Gross total resection (GTR) was achieved in 50 patients (71%). Tissue was processed for next-generation sequencing in 64 cases (91%), and for DNA methylation analysis in 58 cases (83%), while immunohistochemistry for mTOR phosphorylation was performed in 24 cases (34%). Targeted therapy was recommended in 35 (50%) and commenced in 21 (30%) cases. Postoperatively, 7 patients (11%) required revision surgery, compared to 7% (p = 0.519) and 6% (p = 0.359) of our reference cohorts of patients undergoing first and second craniotomy, respectively. Non-resolving neurological deterioration was documented in 6 cases (10% vs. 8%, p = 0.612, after first and 4%, p = 0.519, after second craniotomy). Median survival after repeat surgery was 399 days in all patients and 348 days in GBM patients after repeat GTR.
Surgery for recurrent glioma provides relevant molecular diagnostic information with a direct consequence for targeted therapy under a reasonable risk of postoperative complications. With satisfactory postoperative survival it can therefore complement a multi-modal glioma therapy approach.
复发性神经胶质瘤的手术可提供细胞减灭术和用于分子指导治疗的组织。由于涉及的患者大多经过大量预处理,因此尚不清楚重复手术的益处是否超过其潜在风险。
回顾性分析了因靶向治疗目的而接受复发性 2-4 级神经胶质瘤手术的患者。比较了手术并发症(手术、神经学)率与本机构神经胶质瘤手术队列。分析了组织分子诊断产量、靶向治疗和术后生存率。
在 2017 年至 2022 年间,肿瘤委员会建议通过分子诊断对 180 名患者进行靶向治疗。其中,70 名患者(38%)接受了重复手术。诊断为 IDH 野生型胶质母细胞瘤 48 例(69%),其次为 IDH 突变型星形细胞瘤 13 例(19%)和少突胶质细胞瘤 9 例(13%)。50 例(71%)患者实现了大体全切除(GTR)。64 例(91%)进行了下一代测序处理,58 例(83%)进行了 DNA 甲基化分析,24 例(34%)进行了 mTOR 磷酸化免疫组化检测。35 例(50%)推荐靶向治疗,并开始 21 例(30%)。术后,7 例(11%)需要再次手术,而首次开颅手术的参考队列中有 7%(p=0.519)和第二次开颅手术的参考队列中有 6%(p=0.359)需要再次手术。6 例(10%)记录到无法缓解的神经功能恶化,与首次开颅后 8%(p=0.612)和第二次开颅后 4%(p=0.519)相比。所有患者重复手术后的中位生存时间为 399 天,重复 GTR 后的 GBM 患者为 348 天。
复发性神经胶质瘤的手术可提供相关的分子诊断信息,直接影响靶向治疗,且术后并发症风险合理。具有令人满意的术后生存,因此可以补充多模式神经胶质瘤治疗方法。