Department of Emergency Medicine, University of Washington, Seattle, WA, United States.
Department of Global Health, University of Washington, Seattle, WA, United States.
Front Public Health. 2024 Jan 30;11:1324636. doi: 10.3389/fpubh.2023.1324636. eCollection 2023.
Data on ethnic and racial differences in symptoms and health-related impacts following SARS-CoV-2 infection are limited. We aimed to estimate the ethnic and racial differences in symptoms and health-related impacts 3 and 6 months after the first SARS-CoV-2 infection.
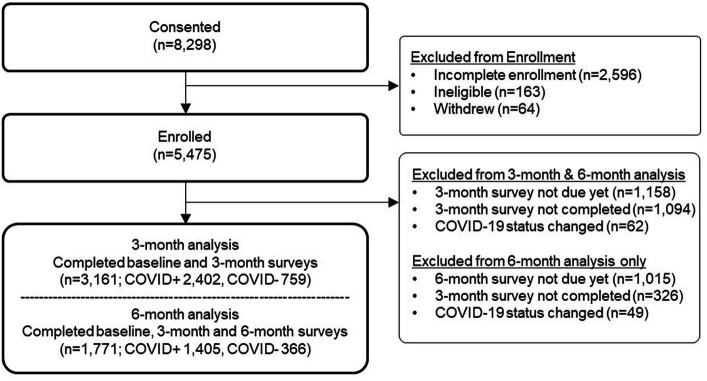
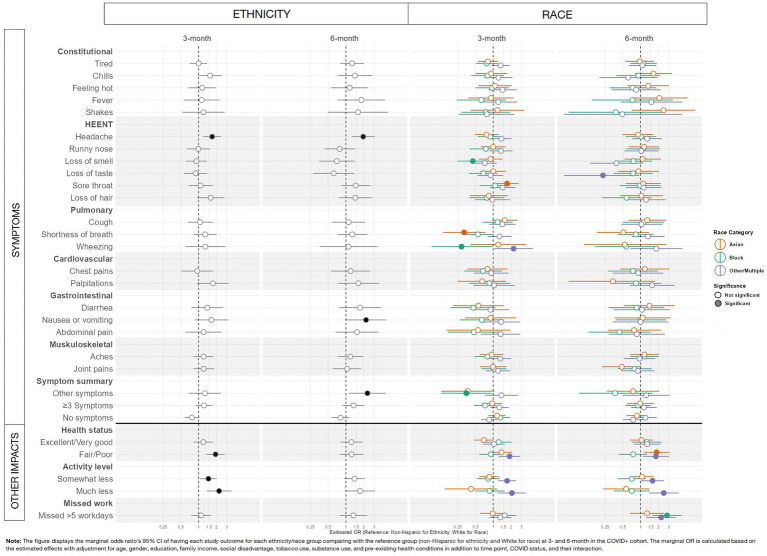
Participants included adults with SARS-CoV-2 infection enrolled in a prospective multicenter US study between 12/11/2020 and 7/4/2022 as the primary cohort of interest, as well as a SARS-CoV-2-negative cohort to account for non-SARS-CoV-2-infection impacts, who completed enrollment and 3-month surveys ( = 3,161; 2,402 SARS-CoV-2-positive, 759 SARS-CoV-2-negative). Marginal odds ratios were estimated using GEE logistic regression for individual symptoms, health status, activity level, and missed work 3 and 6 months after COVID-19 illness, comparing each ethnicity or race to the referent group (non-Hispanic or white), adjusting for demographic factors, social determinants of health, substance use, pre-existing health conditions, SARS-CoV-2 infection status, COVID-19 vaccination status, and survey time point, with interactions between ethnicity or race and time point, ethnicity or race and SARS-CoV-2 infection status, and SARS-CoV-2 infection status and time point.
Following SARS-CoV-2 infection, the majority of symptoms were similar over time between ethnic and racial groups. At 3 months, Hispanic participants were more likely than non-Hispanic participants to report fair/poor health (OR: 1.94; 95%CI: 1.36-2.78) and reduced activity (somewhat less, OR: 1.47; 95%CI: 1.06-2.02; much less, OR: 2.23; 95%CI: 1.38-3.61). At 6 months, differences by ethnicity were not present. At 3 months, Other/Multiple race participants were more likely than white participants to report fair/poor health (OR: 1.90; 95% CI: 1.25-2.88), reduced activity (somewhat less, OR: 1.72; 95%CI: 1.21-2.46; much less, OR: 2.08; 95%CI: 1.18-3.65). At 6 months, Asian participants were more likely than white participants to report fair/poor health (OR: 1.88; 95%CI: 1.13-3.12); Black participants reported more missed work (OR, 2.83; 95%CI: 1.60-5.00); and Other/Multiple race participants reported more fair/poor health (OR: 1.83; 95%CI: 1.10-3.05), reduced activity (somewhat less, OR: 1.60; 95%CI: 1.02-2.51; much less, OR: 2.49; 95%CI: 1.40-4.44), and more missed work (OR: 2.25; 95%CI: 1.27-3.98).
Awareness of ethnic and racial differences in outcomes following SARS-CoV-2 infection may inform clinical and public health efforts to advance health equity in long-term outcomes.
关于 SARS-CoV-2 感染后症状和与健康相关影响的种族和民族差异的数据有限。我们旨在估计首次 SARS-CoV-2 感染后 3 个月和 6 个月时症状和与健康相关影响的种族和民族差异。
参与者包括 2020 年 12 月 11 日至 2022 年 7 月 4 日期间在美国一项前瞻性多中心研究中感染 SARS-CoV-2 的成年人,以及为了说明非 SARS-CoV-2 感染影响而纳入的 SARS-CoV-2 阴性队列,他们完成了入组和 3 个月调查( = 3161;2402 例 SARS-CoV-2 阳性,759 例 SARS-CoV-2 阴性)。使用广义估计方程逻辑回归估计个体症状、健康状况、活动水平和 COVID-19 疾病后 3 个月和 6 个月缺勤的边缘优势比,将每个族裔或种族与参考组(非西班牙裔或白人)进行比较,调整人口统计学因素、健康的社会决定因素、物质使用、预先存在的健康状况、SARS-CoV-2 感染状态、COVID-19 疫苗接种状态和调查时间点,同时考虑种族或民族与时间点、种族或民族与 SARS-CoV-2 感染状态以及 SARS-CoV-2 感染状态与时间点之间的相互作用。
SARS-CoV-2 感染后,大多数症状在不同族裔和种族群体之间随时间变化相似。在 3 个月时,与非西班牙裔参与者相比,西班牙裔参与者更有可能报告健康状况不佳(优势比[OR]:1.94;95%置信区间[CI]:1.36-2.78)和活动减少(有些减少,OR:1.47;95%CI:1.06-2.02;明显减少,OR:2.23;95%CI:1.38-3.61)。在 6 个月时,族裔差异不存在。在 3 个月时,其他/多种族参与者比白人参与者更有可能报告健康状况不佳(OR:1.90;95%CI:1.25-2.88),活动减少(有些减少,OR:1.72;95%CI:1.21-2.46;明显减少,OR:2.08;95%CI:1.18-3.65)。在 6 个月时,亚洲参与者比白人参与者更有可能报告健康状况不佳(OR:1.88;95%CI:1.13-3.12);黑人参与者报告更多缺勤(OR,2.83;95%CI:1.60-5.00);其他/多种族参与者报告更多健康状况不佳(OR:1.83;95%CI:1.10-3.05),活动减少(有些减少,OR:1.60;95%CI:1.02-2.51;明显减少,OR:2.49;95%CI:1.40-4.44),以及更多缺勤(OR:2.25;95%CI:1.27-3.98)。
了解 SARS-CoV-2 感染后结局的种族和民族差异,可能有助于为改善长期结局的临床和公共卫生努力提供信息,以实现健康公平。