NYU Grossman School of Medicine New York NY USA.
Duke Clinical Research Institute Durham NC USA.
J Am Heart Assoc. 2024 Mar 5;13(5):e029850. doi: 10.1161/JAHA.122.029850. Epub 2024 Feb 27.
Women with chronic coronary disease are generally older than men and have more comorbidities but less atherosclerosis. We explored sex differences in revascularization, guideline-directed medical therapy, and outcomes among patients with chronic coronary disease with ischemia on stress testing, with and without invasive management.
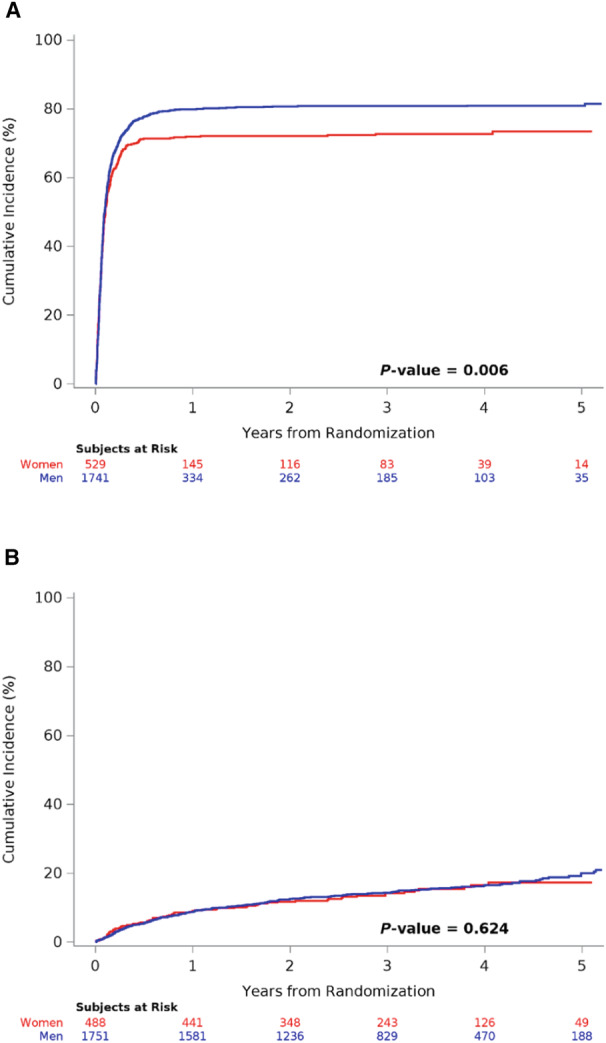
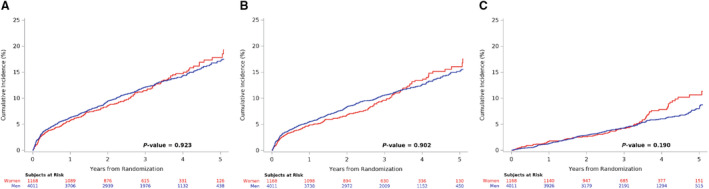
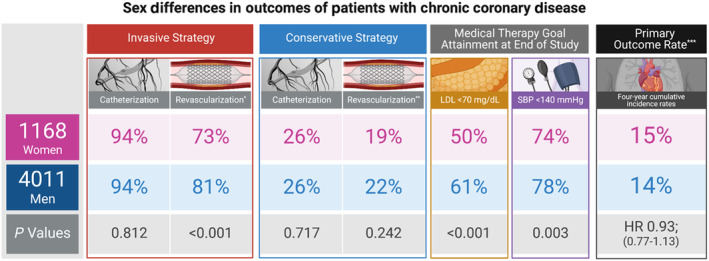
The ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial randomized patients with moderate or severe ischemia to invasive management with angiography, revascularization, and guideline-directed medical therapy, or initial conservative management with guideline-directed medical therapy alone. We evaluated the primary outcome (cardiovascular death, myocardial infarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. Invasive group catheterization rates were similar, with less revascularization among women (73.4% of invasive-assigned women revascularized versus 81.2% of invasive-assigned men; <0.001). Women had less coronary artery disease: multivessel in 60.0% of invasive-assigned women and 74.8% of invasive-assigned men, and no ≥50% stenosis in 12.3% versus 4.5% (<0.001). In the conservative group, 4-year catheterization rates were 26.3% of women versus 25.6% of men (=0.72). Guideline-directed medical therapy use was lower among women with fewer risk factor goals attained. There were no sex differences in the primary outcome (adjusted hazard ratio [HR] for women versus men, 0.93 [95% CI, 0.77-1.13]; =0.47) or the major secondary outcome of cardiovascular death/myocardial infarction (adjusted HR, 0.93 [95% CI, 0.76-1.14]; =0.49), with no significant sex-by-treatment-group interactions.
Women had less extensive coronary artery disease and, therefore, lower revascularization rates in the invasive group. Despite lower risk factor goal attainment, women with chronic coronary disease experienced similar risk-adjusted outcomes to men in the ISCHEMIA trial.
URL: http://wwwclinicaltrials.gov. Unique identifier: NCT01471522.
患有慢性冠状动脉疾病的女性通常比男性年长,且合并症更多,但动脉粥样硬化程度较轻。我们探讨了在压力测试中发现存在缺血但未接受有创治疗或接受有创治疗的慢性冠状动脉疾病患者中,在血运重建、指南指导下的药物治疗和结局方面的性别差异,同时考虑了有创管理和无有创管理两种情况。
ISCHEMIA(国际比较医疗效果与有创和介入治疗研究)试验将中等或重度缺血的患者随机分为接受有创治疗(包括血管造影、血运重建和指南指导下的药物治疗)或初始保守治疗(仅接受指南指导下的药物治疗)。我们按性别评估了 1168 名(22.6%)女性和 4011 名(77.4%)男性患者的主要结局(心血管死亡、心肌梗死或不稳定型心绞痛、心力衰竭或心脏复苏后住院)和其他终点。在接受有创治疗的患者中,女性的导管插入术比例相似,但接受血运重建的比例较低(22.6%的女性接受血运重建,而 81.2%的男性接受血运重建;<0.001)。女性的冠状动脉疾病较轻:22.6%的接受有创治疗的女性和 74.8%的接受有创治疗的男性为多血管病变,无≥50%狭窄的比例为 12.3%和 4.5%(<0.001)。在保守治疗组中,女性的 4 年导管插入术率为 26.3%,男性为 25.6%(=0.72)。接受指南指导下的药物治疗的女性达标率较低,达到的风险因素目标较少。在主要结局(女性的调整后风险比[HR]为 0.93[95%置信区间,0.77-1.13];=0.47)或主要次要结局(心血管死亡/心肌梗死)(调整后 HR,0.93[95%置信区间,0.76-1.14];=0.49)方面,女性与男性之间无性别差异,且治疗组之间无显著的性别交互作用。
与接受有创治疗的女性相比,女性的冠状动脉疾病较轻,因此血运重建率较低。尽管女性达到的风险因素目标较低,但在 ISCHEMIA 试验中,患有慢性冠状动脉疾病的女性与男性的风险调整结局相似。