Zeng Xinyu, Zhang Rui, Jiang Weizhong, Li Chengguo, Yu Minhao, Liu Weizhen, Di Maojun, Wu Hongxue, Sun Yueming, Xiong Zhiguo, Jiang Congqing, Yu Bin, Zhou Shengning, Li Yong, Liao Xiaofeng, Xia Lijian, Zhang Wei, Lin Guole, Tao Kaixiong
Department of Gastrointestinal Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Department of Colorectal Cancer, Liaoning Cancer Hospital & Institute, Shenyang, China.
Dis Colon Rectum. 2024 Jul 1;67(7):911-919. doi: 10.1097/DCR.0000000000003097. Epub 2024 Mar 7.
Studies on grade 2 rectal neuroendocrine tumors are limited, and the optimal treatment for these tumors is not well established.
We aimed to compare the oncologic results of local excision versus radical resection for the treatment of grade 2 rectal neuroendocrine tumors.
Retrospective multicenter propensity score-matched study to minimize heterogeneity between groups and focus on the differences between surgery strategies.
Seventeen large-scale Chinese medical centers participated in this study.
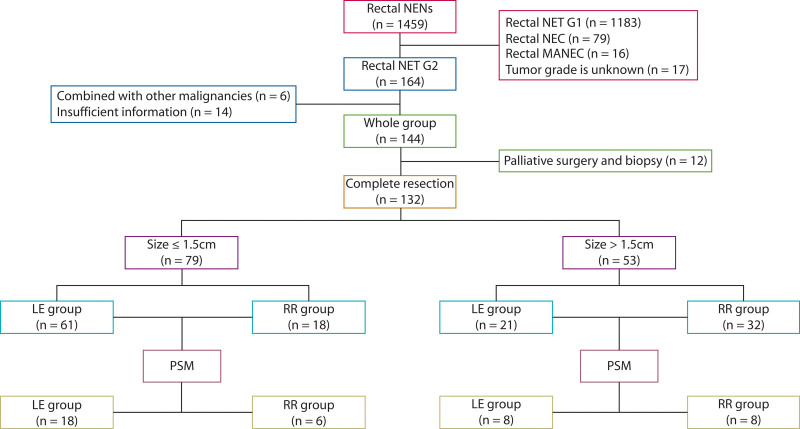
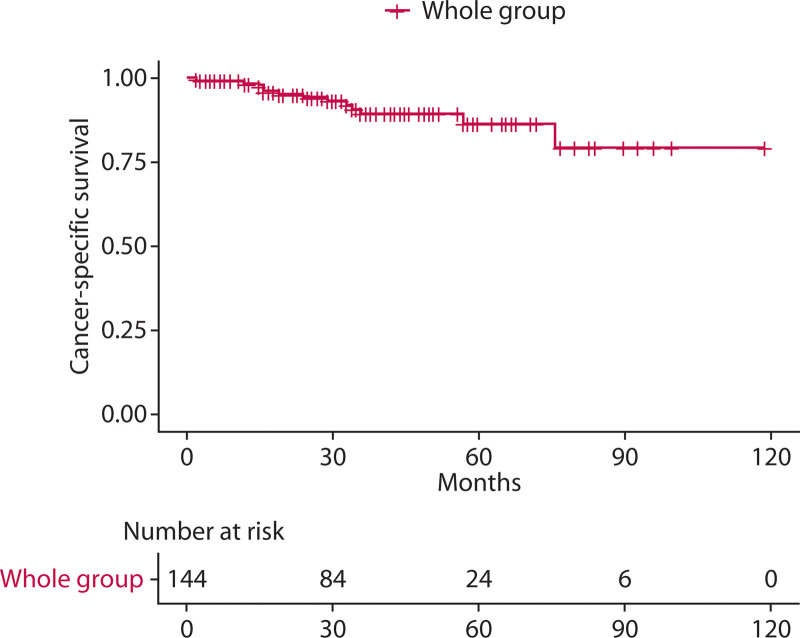
A total of 144 patients with pathologically confirmed grade 2 rectal neuroendocrine tumors were retrospectively analyzed.
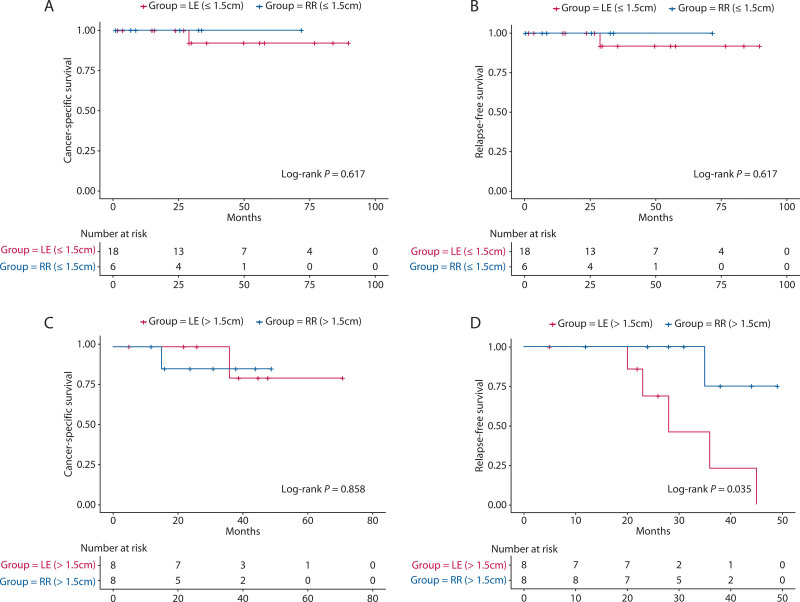
Cancer-specific survival and relapse-free survival were assessed to compare surgery strategies.
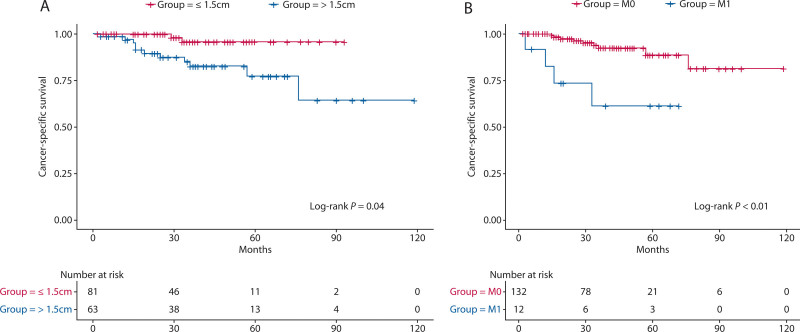
A total of 144 patients with grade 2 rectal neuroendocrine tumors were enrolled in this study. Twenty-seven patients underwent endoscopic resection, 55 underwent transanal excision, 50 underwent radical resection, and 12 underwent palliative surgery or biopsy for distant metastasis. Of the 50 patients who underwent radical resection, 30 (60.0%) had clinically positive lymph nodes on the basis of the histopathology results. The optimal cutoff value for tumor size to predict cancer-specific survival was 1.5 cm. In patients with grade 2 rectal neuroendocrine tumors of ≤1.5-cm size, there were no significant differences in cancer-specific survival and relapse-free survival between local excision and radical resection groups ( p > 0.05). In patients with grade 2 rectal neuroendocrine tumors of >1.5-cm size, relapse-free survival was significantly lower in the local excision group than in the radical resection group ( p = 0.04).
The nature of retrospective reviews and a relatively short follow-up period are limitations of this study.
Grade 2 rectal neuroendocrine tumors have a nonnegligible rate of lymph node metastasis. Local excision is a feasible choice for tumors of ≤1.5 cm size without metastasis, whereas radical resection is more beneficial in those of >1.5 cm size. See Video Abstract .
ANTECEDENTES:Los estudios sobre los tumores neuroendocrinos rectales de grado 2 son limitados y el tratamiento óptimo para estos tumores no está bien establecido.OBJETIVO:Comparar los resultados oncológicos de la escisión local versus la resección radical para el tratamiento de tumores neuroendocrinos rectales grado 2.DISEÑO:Estudio multicéntrico retrospectivo emparejado por puntuación de propensión para minimizar la heterogeneidad entre grupos y centrarse en la diferencia entre estrategias quirúrgicas.ESCENARIO:Diecisiete centros médicos chinos de gran tamaño participaron en este estudio.PACIENTES:Se analizaron retrospectivamente un total de 144 pacientes con tumores neuroendocrinos rectales grado 2 patológicamente confirmados.PRINCIPALES MEDIDAS DE RESULTADO:Se evaluaron la supervivencia específica del cáncer y la supervivencia libre de recaída para comparar las estrategias quirúrgicas.RESULTADOS:En este estudio se inscribieron un total de 144 pacientes con tumores neuroendocrinos rectales grado 2. Veintisiete pacientes se sometieron a resección endoscópica, 55 a escisión transanal, 50 a resección radical y 12 a cirugía paliativa o biopsia por metástasis a distancia. De los 50 pacientes que se sometieron a resección radical, 30 (60,0%) tenían ganglios linfáticos clínicamente positivos según los resultados histopatológicos. El valor de corte óptimo para el tamaño del tumor para predecir la supervivencia específica del cáncer fue de 1,5 cm. En pacientes con tumores neuroendocrinos rectales grado 2 ≤ 1,5 cm, no hubo diferencias significativas en la supervivencia específica del cáncer y la supervivencia libre de recaída entre los grupos de escisión local y resección radical ( p >0,05). En pacientes con tumores neuroendocrinos rectales grado 2 > 1,5 cm, la supervivencia libre de recaída fue significativamente menor en el grupo de escisión local que en el grupo de resección radical ( p = 0,04).LIMITACIONES:La naturaleza de la revisión retrospectiva y el período de seguimiento relativamente corto son limitaciones de este estudio.CONCLUSIONES:Los tumores neuroendocrinos rectales grado 2 tienen una tasa no despreciable de metástasis en los ganglios linfáticos. La escisión local es una opción factible para tumores ≤ 1,5 cm sin metástasis, mientras que la resección radical es más beneficiosa en aquellos > 1,5 cm. (Traducción-Dr. Felipe Bellolio ).
关于2级直肠神经内分泌肿瘤的研究有限,这些肿瘤的最佳治疗方法尚未明确确立。
我们旨在比较局部切除与根治性切除治疗2级直肠神经内分泌肿瘤的肿瘤学结果。
回顾性多中心倾向评分匹配研究,以尽量减少组间异质性,并关注手术策略之间的差异。
17家大型中国医疗中心参与了本研究。
共回顾性分析了144例经病理证实的2级直肠神经内分泌肿瘤患者。
评估癌症特异性生存率和无复发生存率以比较手术策略。
本研究共纳入144例2级直肠神经内分泌肿瘤患者。27例患者接受了内镜切除,55例接受了经肛门切除,50例接受了根治性切除,12例因远处转移接受了姑息性手术或活检。在接受根治性切除的50例患者中,根据组织病理学结果,30例(60.0%)临床淋巴结阳性。预测癌症特异性生存的肿瘤大小最佳截断值为1.5 cm。在肿瘤大小≤1.5 cm的2级直肠神经内分泌肿瘤患者中,局部切除组和根治性切除组的癌症特异性生存率和无复发生存率无显著差异(p>0.05)。在肿瘤大小>1.5 cm的2级直肠神经内分泌肿瘤患者中,局部切除组的无复发生存率显著低于根治性切除组(p=0.04)。
回顾性研究的性质和相对较短的随访期是本研究的局限性。
2级直肠神经内分泌肿瘤的淋巴结转移率不可忽视。对于大小≤1.5 cm且无转移的肿瘤,局部切除是一种可行的选择,而对于大小>1.5 cm的肿瘤,根治性切除更有益。见视频摘要。
背景:关于2级直肠神经内分泌肿瘤的研究有限,这些肿瘤的最佳治疗方法尚未明确确立。目的:比较局部切除与根治性切除治疗2级直肠神经内分泌肿瘤的肿瘤学结果。设计:回顾性多中心倾向评分匹配研究,以尽量减少组间异质性,并关注手术策略之间的差异。背景:17家大型中国医疗中心参与了本研究。患者:共回顾性分析了144例经病理证实的2级直肠神经内分泌肿瘤患者。主要观察指标:评估癌症特异性生存率和无复发生存率以比较手术策略。结果:本研究共纳入144例2级直肠神经内分泌肿瘤患者。27例患者接受了内镜切除,55例接受了经肛门切除,50例接受了根治性切除,12例因远处转移接受了姑息性手术或活检。在接受根治性切除的50例患者中,根据组织病理学结果,30例(60.0%)临床淋巴结阳性。预测癌症特异性生存的肿瘤大小最佳截断值为1.5 cm。在肿瘤大小≤1.5 cm的2级直肠神经内分泌肿瘤患者中,局部切除组和根治性切除组的癌症特异性生存率和无复发生存率无显著差异(p>0.05)。在肿瘤大小>1.5 cm的2级直肠神经内分泌肿瘤患者中,局部切除组的无复发生存率显著低于根治性切除组(p=0.04)。局限性:回顾性研究的性质和相对较短的随访期是本研究的局限性。结论:2级直肠神经内分泌肿瘤的淋巴结转移率不可忽视。对于大小≤1.5 cm且无转移的肿瘤,局部切除是一种可行的选择,而对于大小>1.5 cm的肿瘤,根治性切除更有益。(翻译 - 费利佩·贝洛利奥医生)