Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway.
Prehospital affiliationision, Oslo University Hospital, Oslo, Norway.
BMC Emerg Med. 2024 Mar 14;24(1):43. doi: 10.1186/s12873-024-00962-7.
In this study we aimed to explore EMCC triage of suspected and confirmed stroke patients to gain more knowledge about the initial phase of the acute stroke response chain. Accurate dispatch at the Emergency Medical Communication Center (EMCC) is crucial for optimal resource utilization in the prehospital service, and early identification of acute stroke is known to improve patient outcome.
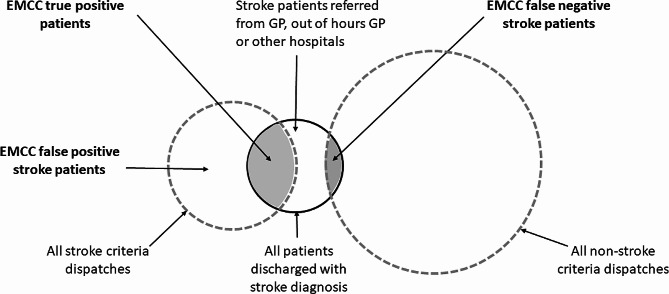
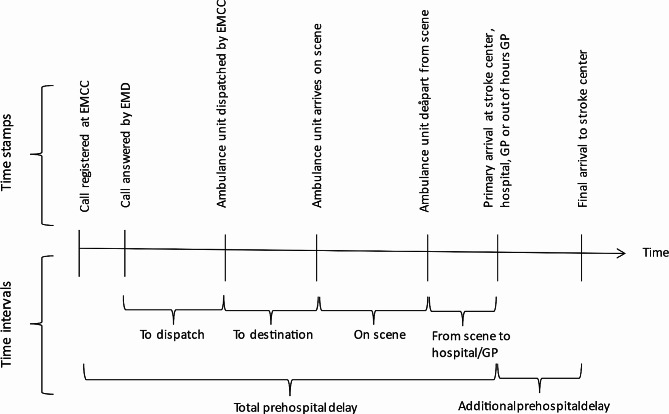
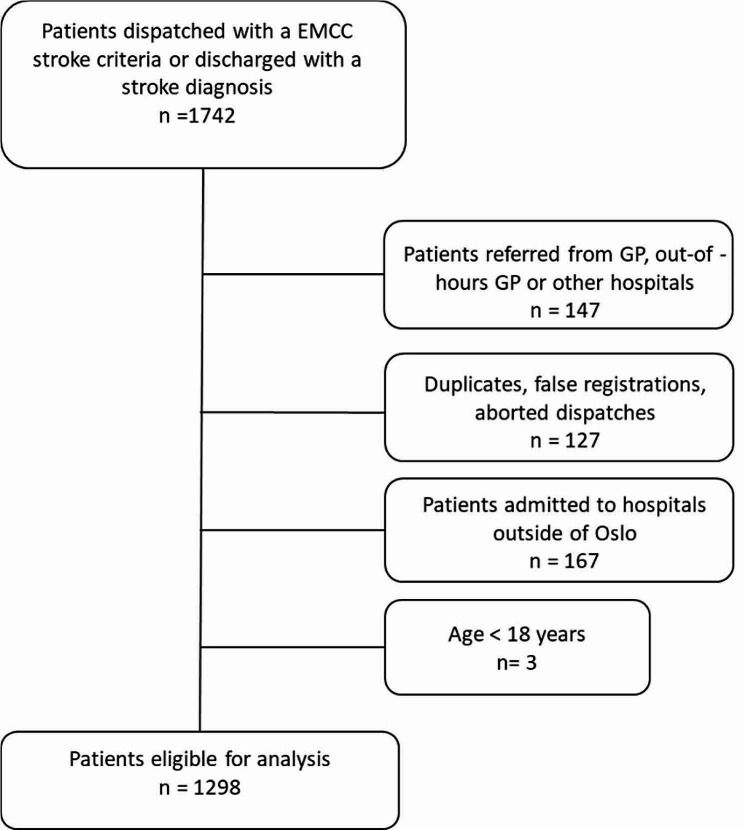
We conducted a descriptive retrospective study based on data from the Emergency Department and EMCC records at a comprehensive stroke center in Oslo, Norway, during a six-month period (2019-2020). Patients dispatched with EMCC stroke criteria and/or discharged with a stroke diagnosis were included. We identified EMCC true positive, false positive and false negative stroke patients and estimated EMCC stroke sensitivity and positive predictive value (PPV). Furthermore, we analyzed prehospital time intervals and identified patient destinations to gain knowledge on ambulance services assessments.
We included 1298 patients. EMCC stroke sensitivity was 77% (95% CI: 72 - 82%), and PPV was 16% (95% CI: 14 - 18%). EMCC false negative stroke patients experienced an increased median prehospital delay of 11 min (p < 0.001). Upon arrival at the scene, 68% of the EMCC false negative patients were identified as suspected stroke cases by the ambulance services. Similarly, 68% of the false positive stroke patients were either referred to a GP, out-of-hours GP acute clinic, local hospitals or left at the scene by the ambulance services, indicating that no obvious stroke symptoms were identified by ambulance personnel upon arrival at the scene.
This study reveals a high EMCC stroke sensitivity and an extensive number of false positive stroke dispatches. By comparing the assessments made by both the EMCC and the ambulance service, we have identified specific patient groups that should be the focus for future research efforts aimed at improving the sensitivity and specificity of stroke recognition in the EMCC.
本研究旨在探讨紧急医疗通讯中心(EMCC)对疑似和确诊脑卒中患者的分诊,以更多地了解急性脑卒中反应链的初始阶段。在院前服务中,EMCC 的准确调度对于优化资源利用至关重要,而早期识别急性脑卒中可改善患者预后。
我们进行了一项描述性回顾性研究,基于挪威奥斯陆综合卒中中心急诊和 EMCC 记录的数据,研究期间为六个月(2019-2020 年)。将符合 EMCC 卒中标准并被派往 EMCC 或被诊断为卒中后出院的患者纳入研究。我们确定了 EMCC 的真阳性、假阳性和假阴性脑卒中患者,并估计了 EMCC 的脑卒中敏感性和阳性预测值(PPV)。此外,我们分析了院前时间间隔,并确定了患者去向,以了解对救护车服务评估的认识。
我们纳入了 1298 名患者。EMCC 的脑卒中敏感性为 77%(95%CI:72-82%),PPV 为 16%(95%CI:14-18%)。EMCC 的假阴性脑卒中患者经历了 11 分钟中位数增加的院前延迟(p<0.001)。在现场,68%的 EMCC 假阴性患者被救护车服务识别为疑似脑卒中病例。同样,68%的假阳性脑卒中患者被救护车服务转诊至全科医生、夜间全科医生急性诊所、当地医院或留在现场,表明救护车人员在到达现场时未识别出明显的脑卒中症状。
本研究揭示了 EMCC 脑卒中高敏感性和广泛的假阳性脑卒中派遣。通过比较 EMCC 和救护车服务的评估,我们确定了一些特定的患者群体,这些群体应该是未来旨在提高 EMCC 中脑卒中识别的敏感性和特异性的研究重点。