Gastroenterology and Digestive Endoscopy Unit, Fondazione IRCCS Policlinico San Matteo, Viale Camillo Golgi 19, 27100 Pavia, Italy.
Gastroenterology and Digestive Endoscopy Unit, Forlì-Cesena Hospitals, AUSL Romagna, 47121 Forlì, Italy.
Medicina (Kaunas). 2024 Mar 13;60(3):472. doi: 10.3390/medicina60030472.
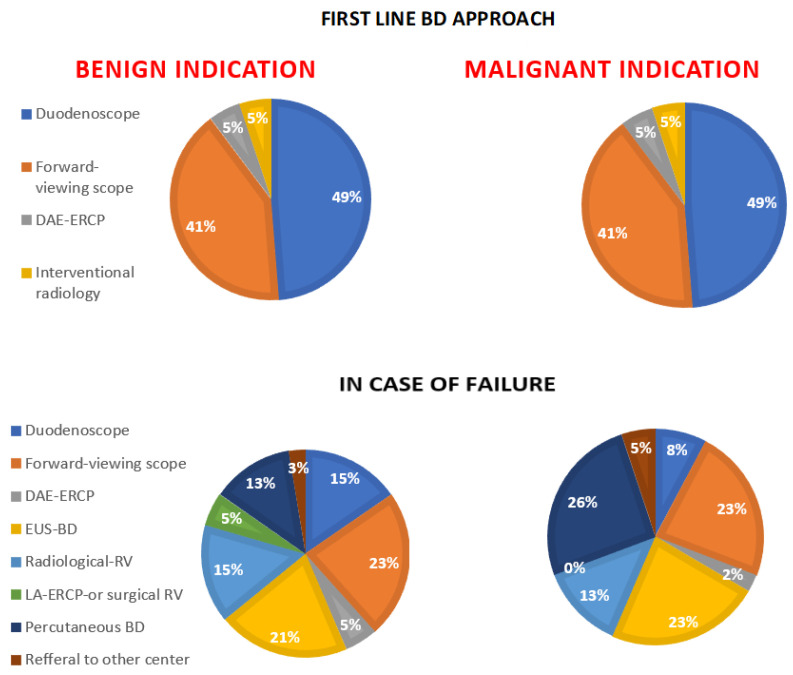
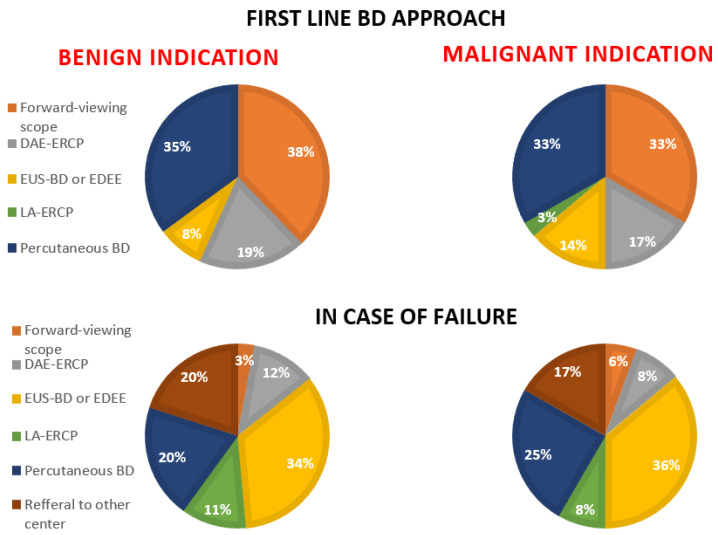
: Biliary drainage (BD) in patients with surgically altered anatomy (SAA) could be obtained endoscopically with different techniques or with a percutaneous approach. Every endoscopic technique could be challenging and not clearly superior over another. The aim of this survey is to explore which is the standard BD approach in patients with SAA. : A 34-question online survey was sent to different Italian tertiary and non-tertiary endoscopic centers performing interventional biliopancreatic endoscopy. The core of the survey was focused on the first-line and alternative BD approaches to SAA patients with benign or malignant obstruction. : Out of 70 centers, 39 answered the survey (response rate: 56%). Only 48.7% of them declared themselves to be reference centers for endoscopic BD in SAA. The total number of procedures performed per year is usually low, especially in non-tertiary centers; however, they have a low tendency to refer to more experienced centers. In the case of Billroth-II reconstruction, the majority of centers declared that they use a duodenoscope or forward-viewing scope in both benign and malignant diseases as a first approach. However, in the case of failure, the BD approach becomes extremely heterogeneous among centers without any technique prevailing over the others. Interestingly, in the case of Roux-en-Y, a significant proportion of centers declared that they choose the percutaneous approach in both benign (35.1%) and malignant obstruction (32.4%) as a first option. In the case of a previous failed attempt at BD in Roux-en-Y, the subsequent most used approach is the EUS-guided intervention in both benign and malignant indications. : This survey shows that the endoscopic BD approach is extremely heterogeneous, especially in patients with Roux-en-Y reconstruction or after ERCP failure in Billroth-II reconstruction. Percutaneous BD is still taken into account by a significant proportion of centers in the case of Roux-en-Y anatomy. The total number of endoscopic BD procedures performed in non-tertiary centers is usually low, but this result does not correspond to an adequate rate of referral to more experienced centers.
: 在解剖结构改变(SAA)的患者中,可以通过不同的技术或经皮途径进行胆道引流(BD)。每种内镜技术都可能具有挑战性,并且不能明显优于另一种。本调查的目的是探讨 SAA 患者的标准 BD 方法。 : 一项 34 个问题的在线调查被发送到不同的意大利三级和非三级内镜中心,进行介入性胰胆内镜检查。该调查的核心集中在 SAA 良性或恶性梗阻患者的一线和替代 BD 方法上。 : 在 70 个中心中,有 39 个回答了调查(应答率:56%)。只有 48.7%的中心表示自己是 SAA 内镜 BD 的参考中心。每年进行的手术总数通常较低,尤其是在非三级中心;然而,他们很少倾向于向更有经验的中心转诊。在毕罗氏Ⅱ型重建的情况下,大多数中心表示,他们在良性和恶性疾病中都使用十二指肠镜或前视镜作为首选方法。然而,一旦失败,BD 方法在各个中心之间变得非常多样化,没有任何一种技术占主导地位。有趣的是,在 Roux-en-Y 的情况下,相当一部分中心表示,他们在良性(35.1%)和恶性梗阻(32.4%)中都选择经皮途径作为首选方法。在 Roux-en-Y 中 BD 尝试失败后,随后最常用的方法是在良性和恶性适应证中进行 EUS 引导的介入。 : 本调查显示,内镜 BD 方法非常多样化,特别是在 Roux-en-Y 重建或毕罗氏Ⅱ型重建中 ERCP 失败的患者中。在 Roux-en-Y 解剖结构的情况下,相当一部分中心仍考虑经皮 BD。非三级中心进行的内镜 BD 手术总数通常较低,但这一结果并不对应于向更有经验的中心转诊的适当比例。