Division of Hematology, University of Washington, Seattle.
now with Dana-Farber Cancer Institute, Boston, Massachusetts.
JAMA Netw Open. 2024 Apr 1;7(4):e244898. doi: 10.1001/jamanetworkopen.2024.4898.
Gastrointestinal stromal tumor (GIST) is a rare cancer treated with the tyrosine kinase inhibitors imatinib mesylate or sunitinib malate. In general, in low- and middle-income countries (LMICs), access to these treatments is limited.
To describe the demographic characteristics, treatment duration, and survival of patients with GIST in LMICs treated with imatinib and sunitinib through The Max Foundation programs.
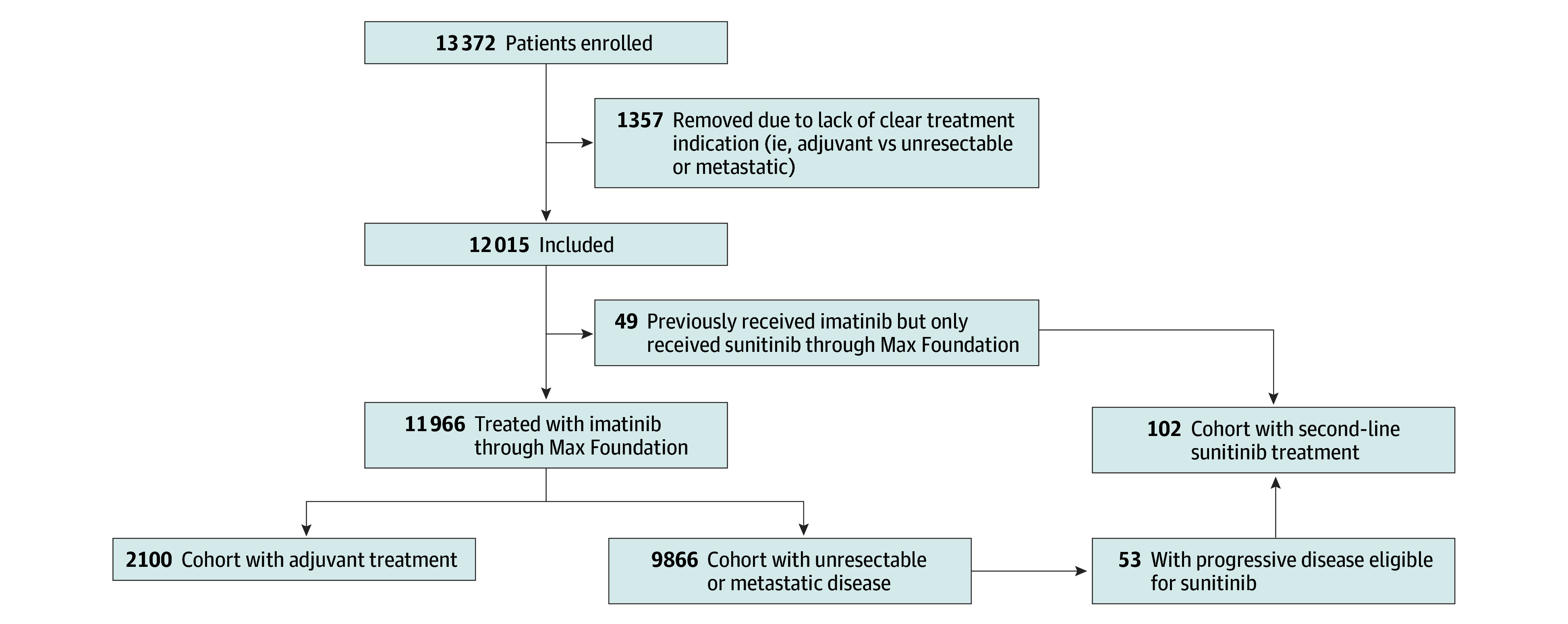
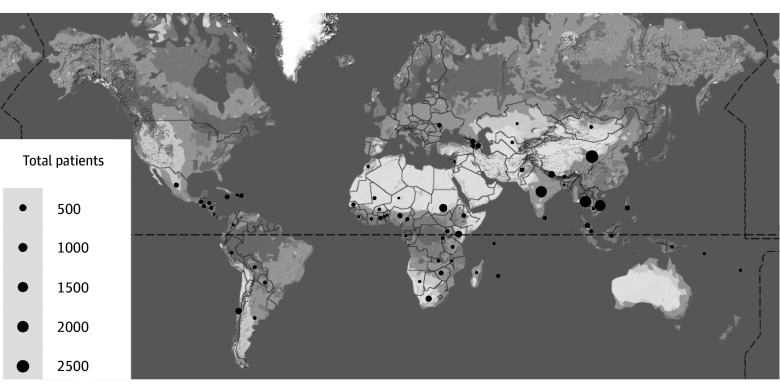
DESIGN, SETTING, AND PARTICIPANTS: This retrospective database cohort analysis included patients in 2 access programs administered by The Max Foundation: the Glivec International Patient Assistance Program (GIPAP), from January 1, 2001, to December 31, 2016, and the Max Access Solutions (MAS) program, January 1, 2017, to October 12, 2020. Sixty-six countries in which The Max Foundation facilitates access to imatinib and sunitinib were included. Participants consisted of patients with approved indications for imatinib, including adjuvant therapy in high-risk GIST by pathologic evaluation of resected tumor or biopsy-proven unresectable or metastatic GIST. All patients were reported to have tumors positive for CD117(c-kit) by treating physicians. A total of 9866 patients received treatment for metastatic and/or unresectable disease; 2100 received adjuvant imatinib; 49 received imatinib from another source and were only included in the sunitinib analysis; and 53 received both imatinib and sunitinib through The Max Foundation programs. Data were analyzed from October 13, 2020, to January 30, 2024.
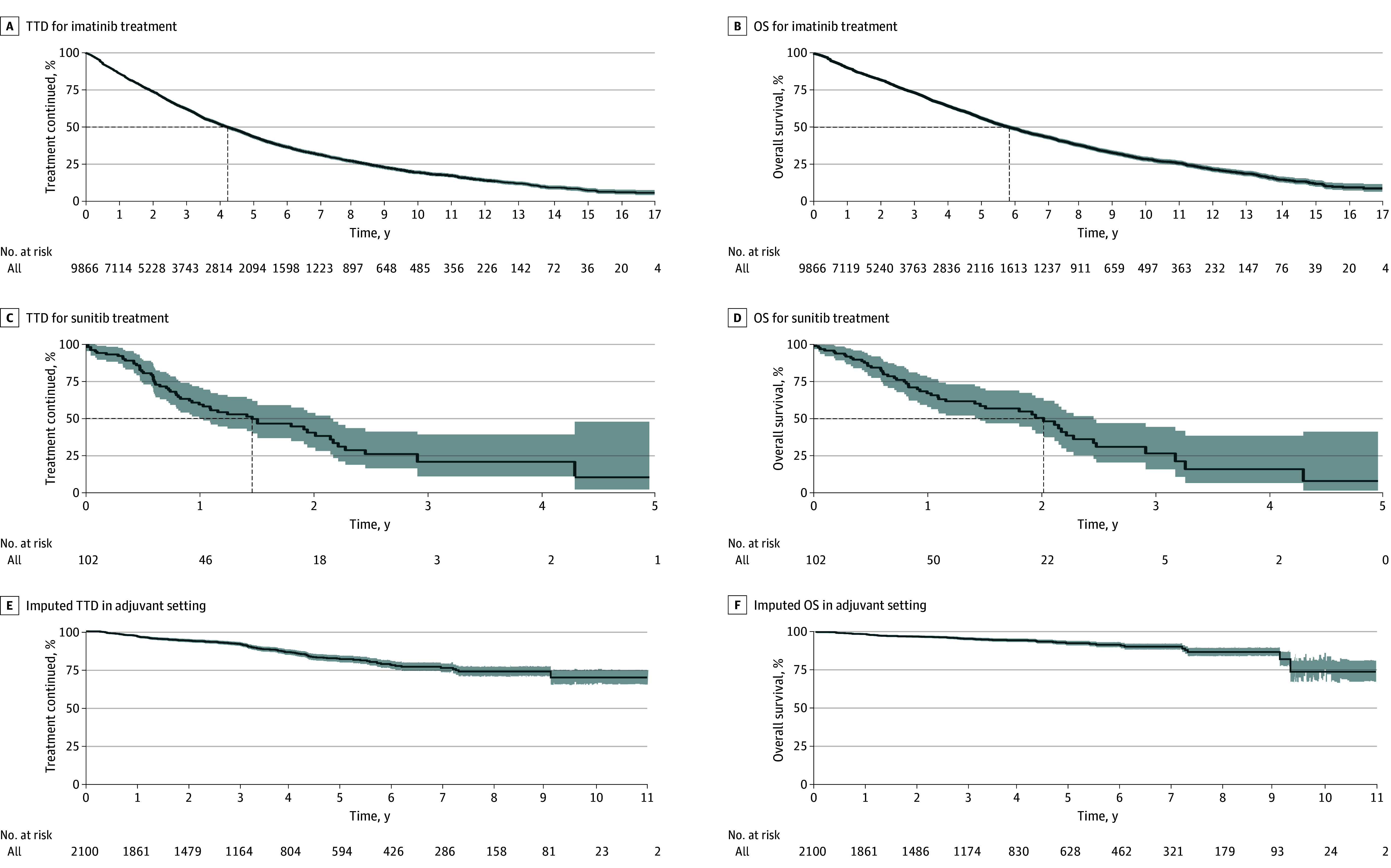
Demographic and clinical information was reported by treating physicians. Kaplan-Meier analysis was used to estimate time to treatment discontinuation (TTD) and overall survival (OS). An imputation-based informed censoring model estimated events for patients lost to follow-up after treatment with adjuvant imatinib. Patients who were lost to follow-up with metastatic or unresectable disease were presumed deceased.
A total of 12 015 unique patients were included in the analysis (6890 male [57.6%]; median age, 54 [range, 0-100] years). Of these, 2100 patients were treated with imatinib in the adjuvant setting (median age, 54 [range 8-88] years) and 9866 were treated with imatinib for metastatic or unresectable disease (median age, 55 [range, 0-100] years). Male patients comprised 5867 of 9866 patients (59.5%) with metastatic or unresectable disease and 1023 of 2100 patients (48.7%) receiving adjuvant therapy. The median OS with imatinib for unresectable or metastatic disease was 5.8 (95% CI, 5.6-6.1) years, and the median TTD was 4.2 (95% CI, 4.1-4.4) years. The median OS with sunitinib for patients with metastatic or unresectable GIST was 2.0 (95% CI, 1.5-2.5) years; the median TTD was 1.5 (95% CI, 1.0-2.1) years. The 10-year OS rate in the adjuvant setting was 73.8% (95% CI, 67.2%-81.1%).
In this cohort study of patients with GIST who were predominantly from LMICs and received orally administered therapy through the GIPAP or MAS programs, outcomes were similar to those observed in high-resource countries. These findings underscore the feasibility and relevance of administering oral anticancer therapy to a molecularly defined population in LMICs, addressing a critical gap in cancer care.
胃肠道间质瘤(GIST)是一种罕见的癌症,用甲磺酸伊马替尼或苹果酸舒尼替尼等酪氨酸激酶抑制剂治疗。一般来说,在中低收入国家(LMICs),这些治疗方法的获得受到限制。
描述通过 The Max Foundation 计划接受甲磺酸伊马替尼和舒尼替尼治疗的 LMICs 中 GIST 患者的人口统计学特征、治疗持续时间和生存情况。
设计、设置和参与者:这项回顾性数据库队列分析包括 The Max Foundation 管理的两个获得途径计划中的患者:Glivec 国际患者援助计划(GIPAP),从 2001 年 1 月 1 日至 2016 年 12 月 31 日,以及 Max 访问解决方案(MAS)计划,从 2017 年 1 月 1 日至 2020 年 10 月 12 日。共有 66 个国家通过 The Max Foundation 获得伊马替尼和舒尼替尼的途径。参与者包括有伊马替尼适应证的患者,包括通过切除肿瘤的病理评估或经活检证实无法切除或转移性 GIST 进行辅助治疗。所有患者的治疗医生报告说肿瘤 CD117(c-kit)阳性。共有 9866 名患者接受转移性和/或不可切除疾病的治疗;2100 名接受辅助伊马替尼治疗;49 名接受来自其他来源的伊马替尼治疗,仅纳入舒尼替尼分析;53 名患者通过 The Max Foundation 计划同时接受伊马替尼和舒尼替尼治疗。数据于 2020 年 10 月 13 日至 2024 年 1 月 30 日进行分析。
治疗医生报告了人口统计学和临床信息。使用 Kaplan-Meier 分析估计治疗停药时间(TTD)和总生存(OS)。基于信息校正的知情删失模型估计了接受辅助伊马替尼治疗后失访的患者的事件。转移性或不可切除疾病的失访患者被假定死亡。
共有 12015 名患者纳入分析(男性 6890 名[57.6%];中位年龄,54 岁[范围,0-100]岁)。其中,2100 名患者接受伊马替尼辅助治疗(中位年龄,54 岁[范围 8-88]岁),9866 名患者接受伊马替尼治疗转移性或不可切除疾病(中位年龄,55 岁[范围,0-100]岁)。转移性或不可切除疾病的 9866 名患者中,男性患者占 5867 名(59.5%),接受辅助治疗的 2100 名患者中,男性患者占 1023 名(48.7%)。不可切除或转移性疾病患者接受伊马替尼治疗的中位 OS 为 5.8 年(95%CI,5.6-6.1 年),中位 TTD 为 4.2 年(95%CI,4.1-4.4 年)。转移性或不可切除 GIST 患者接受舒尼替尼治疗的中位 OS 为 2.0 年(95%CI,1.5-2.5 年);中位 TTD 为 1.5 年(95%CI,1.0-2.1 年)。辅助治疗的 10 年 OS 率为 73.8%(95%CI,67.2%-81.1%)。
在这项队列研究中,患者主要来自中低收入国家,通过 GIPAP 或 MAS 计划接受口服治疗,结果与高资源国家观察到的结果相似。这些发现强调了在中低收入国家对分子定义人群进行口服抗癌治疗的可行性和相关性,解决了癌症护理的一个关键差距。