Department of Oncology, Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
New Zealand Liver Transplant Unit, University of Auckland, Auckland, New Zealand.
Nat Med. 2024 Apr;30(4):1044-1053. doi: 10.1038/s41591-024-02894-y. Epub 2024 Apr 7.
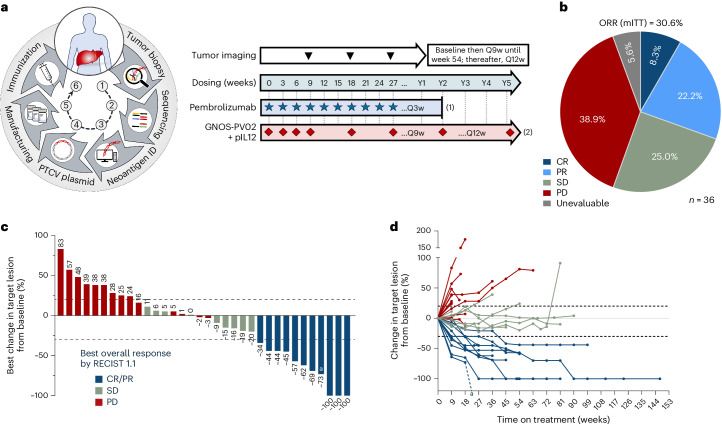
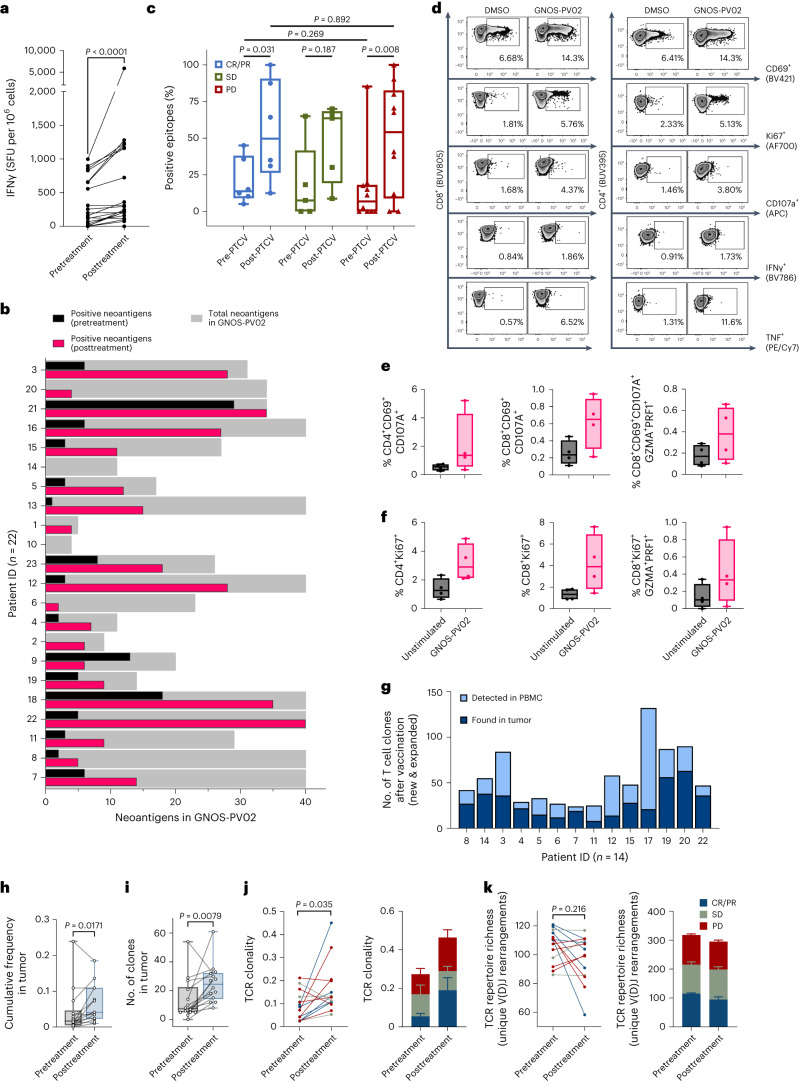
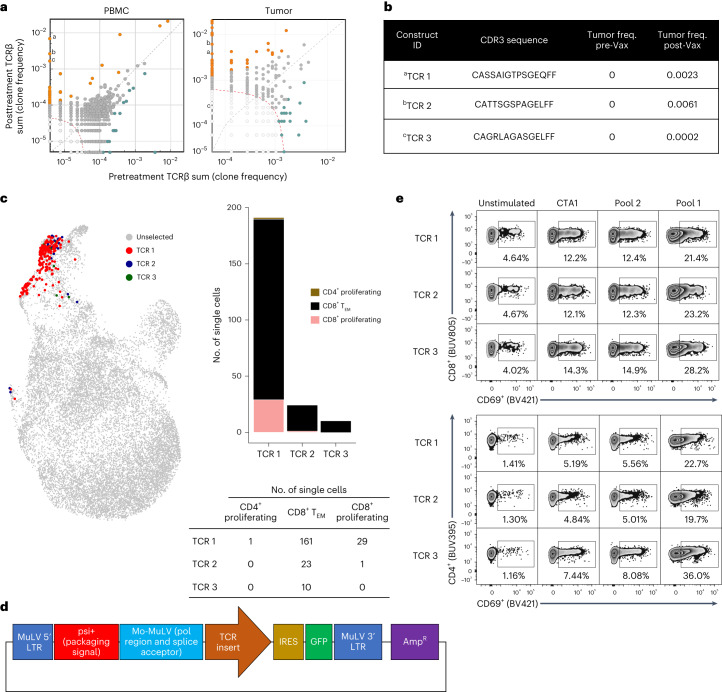
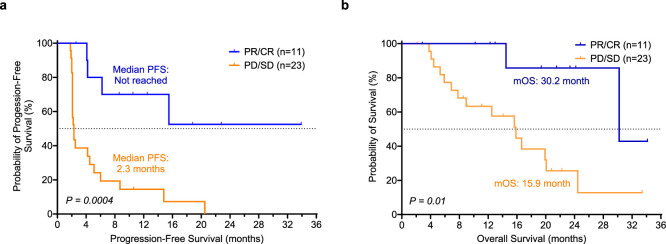
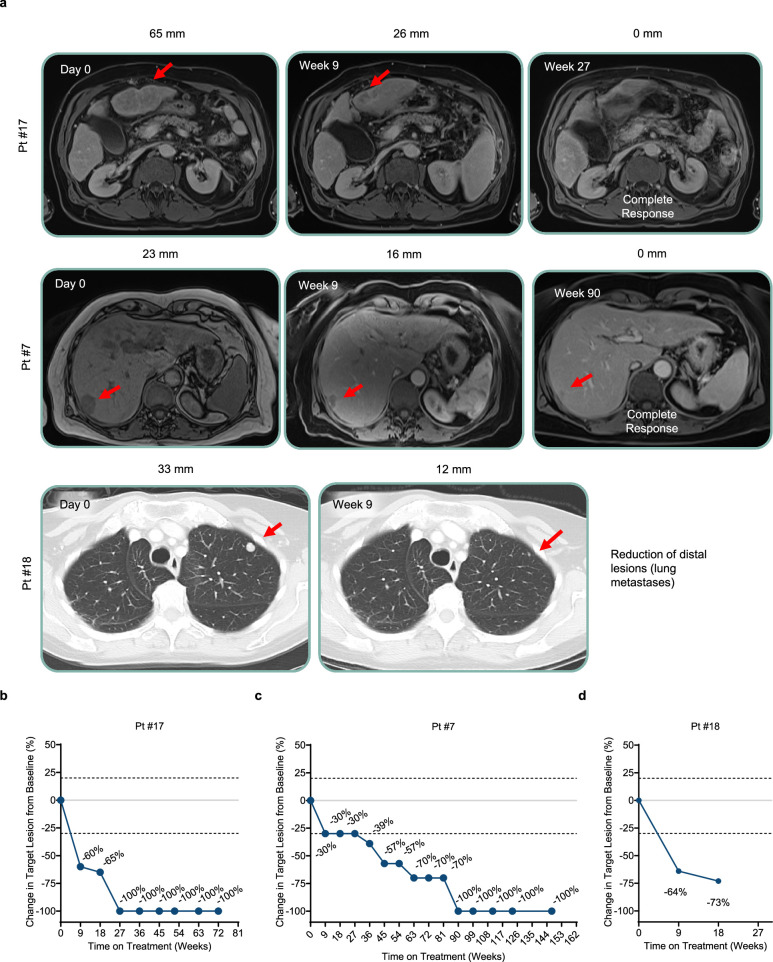
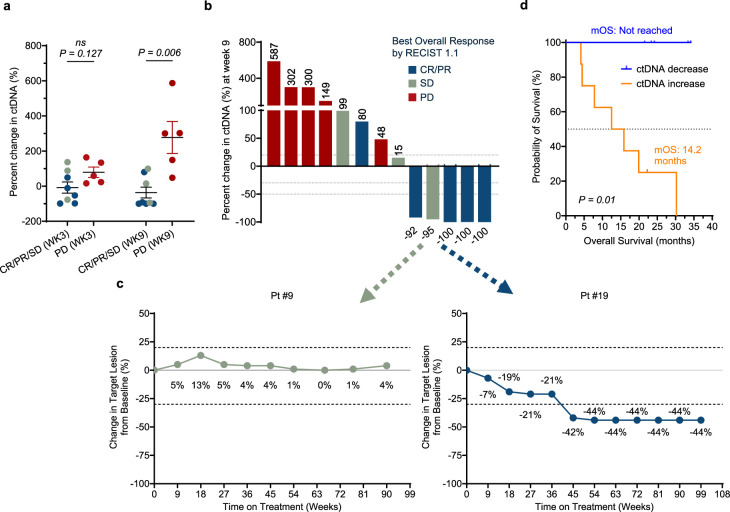
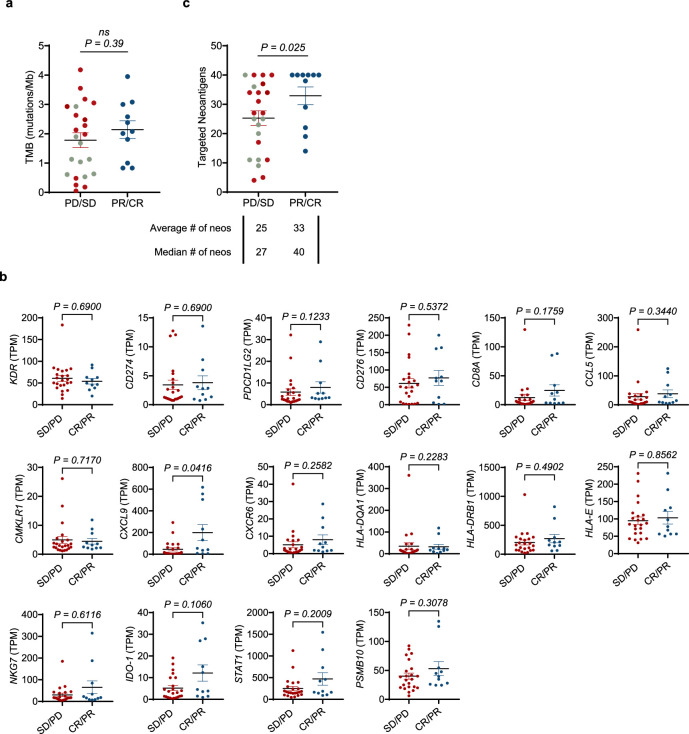
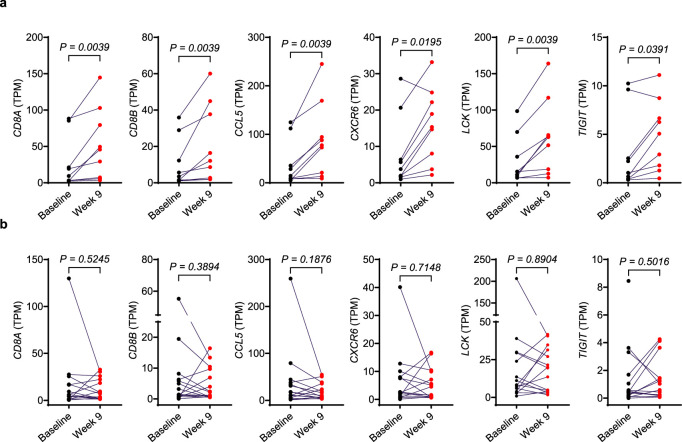
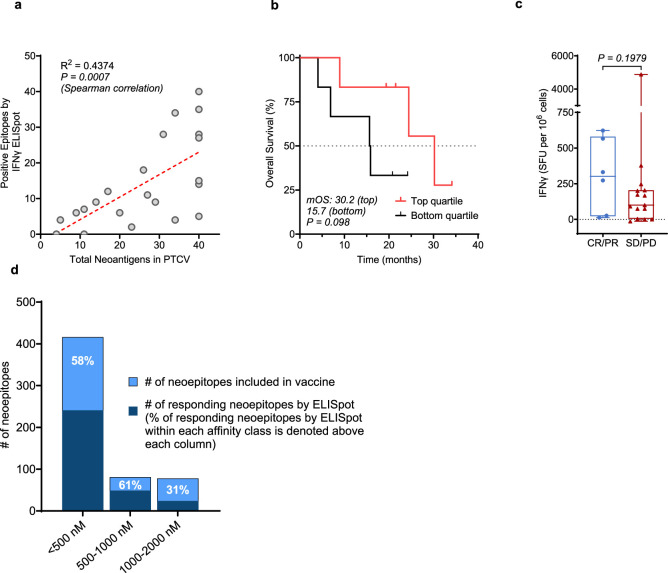
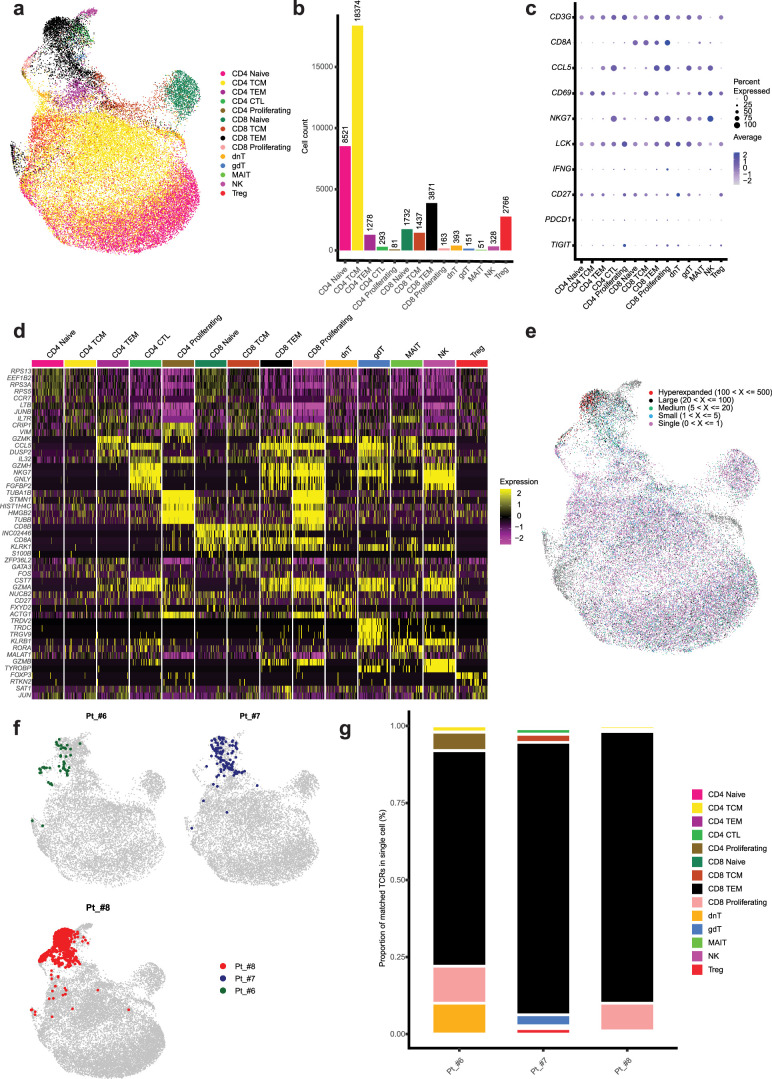
Programmed cell death protein 1 (PD-1) inhibitors have modest efficacy as a monotherapy in hepatocellular carcinoma (HCC). A personalized therapeutic cancer vaccine (PTCV) may enhance responses to PD-1 inhibitors through the induction of tumor-specific immunity. We present results from a single-arm, open-label, phase 1/2 study of a DNA plasmid PTCV (GNOS-PV02) encoding up to 40 neoantigens coadministered with plasmid-encoded interleukin-12 plus pembrolizumab in patients with advanced HCC previously treated with a multityrosine kinase inhibitor. Safety and immunogenicity were assessed as primary endpoints, and treatment efficacy and feasibility were evaluated as secondary endpoints. The most common treatment-related adverse events were injection-site reactions, observed in 15 of 36 (41.6%) patients. No dose-limiting toxicities or treatment-related grade ≥3 events were observed. The objective response rate (modified intention-to-treat) per Response Evaluation Criteria in Solid Tumors 1.1 was 30.6% (11 of 36 patients), with 8.3% (3 of 36) of patients achieving a complete response. Clinical responses were associated with the number of neoantigens encoded in the vaccine. Neoantigen-specific T cell responses were confirmed in 19 of 22 (86.4%) evaluable patients by enzyme-linked immunosorbent spot assays. Multiparametric cellular profiling revealed active, proliferative and cytolytic vaccine-specific CD4 and CD8 effector T cells. T cell receptor β-chain (TCRβ) bulk sequencing results demonstrated vaccination-enriched T cell clone expansion and tumor infiltration. Single-cell analysis revealed posttreatment T cell clonal expansion of cytotoxic T cell phenotypes. TCR complementarity-determining region cloning of expanded T cell clones in the tumors following vaccination confirmed reactivity against vaccine-encoded neoantigens. Our results support the PTCV's mechanism of action based on the induction of antitumor T cells and show that a PTCV plus pembrolizumab has clinical activity in advanced HCC. ClinicalTrials.gov identifier: NCT04251117 .
程序性死亡蛋白 1(PD-1)抑制剂作为单药治疗在肝细胞癌(HCC)中疗效中等。一种个性化治疗性癌症疫苗(PTCV)通过诱导肿瘤特异性免疫,可能增强对 PD-1 抑制剂的反应。我们报告了一项单臂、开放标签、1/2 期研究的结果,该研究使用了一种编码多达 40 个新抗原的 DNA 质粒 PTCV(GNOS-PV02),与质粒编码的白细胞介素-12 联合使用,在先前接受过多酪氨酸激酶抑制剂治疗的晚期 HCC 患者中进行治疗。安全性和免疫原性是主要终点,治疗效果和可行性是次要终点。最常见的治疗相关不良事件是注射部位反应,36 例患者中有 15 例(41.6%)发生。未观察到剂量限制性毒性或治疗相关 3 级及以上事件。根据实体瘤反应评价标准 1.1,客观缓解率(改良意向治疗)为 30.6%(36 例患者中的 11 例),8.3%(36 例患者中的 3 例)的患者完全缓解。临床反应与疫苗中编码的新抗原数量有关。通过酶联免疫斑点分析,在 22 例可评估患者中的 19 例(86.4%)中证实了新抗原特异性 T 细胞反应。多参数细胞分析显示,疫苗特异性 CD4 和 CD8 效应 T 细胞具有活性、增殖和细胞毒性。T 细胞受体β链(TCRβ)批量测序结果表明疫苗接种后 T 细胞克隆扩增和肿瘤浸润。单细胞分析显示治疗后细胞毒性 T 细胞表型的 T 细胞克隆扩增。疫苗接种后肿瘤中扩增的 T 细胞克隆的 TCR 互补决定区克隆证实了对疫苗编码的新抗原的反应性。我们的结果基于诱导抗肿瘤 T 细胞,支持 PTCV 的作用机制,并表明 PTCV 加 pembrolizumab 在晚期 HCC 中有临床活性。临床试验.gov 标识符:NCT04251117。