Dicker Bridget, Garrett Nick, Howie Graham, Brett Aroha, Scott Tony, Stewart Ralph, Perkins Gavin D, Smith Tony, Garcia Elena, Todd Verity F
Clinical Audit and Research, Hato Hone St John New Zealand, Auckland, New Zealand.
Paramedicine Research Unit, Paramedicine Department, Auckland University of Technology, Auckland, New Zealand.
Resusc Plus. 2024 Apr 6;18:100625. doi: 10.1016/j.resplu.2024.100625. eCollection 2024 Jun.
Direct transport to a cardiac arrest centre following out-of-hospital cardiac arrest may be associated with higher survival. However, there is limited evidence available to support this within the New Zealand context. This study used a propensity score-matched cohort to investigate whether direct transport to a cardiac arrest centre improved survival in New Zealand.
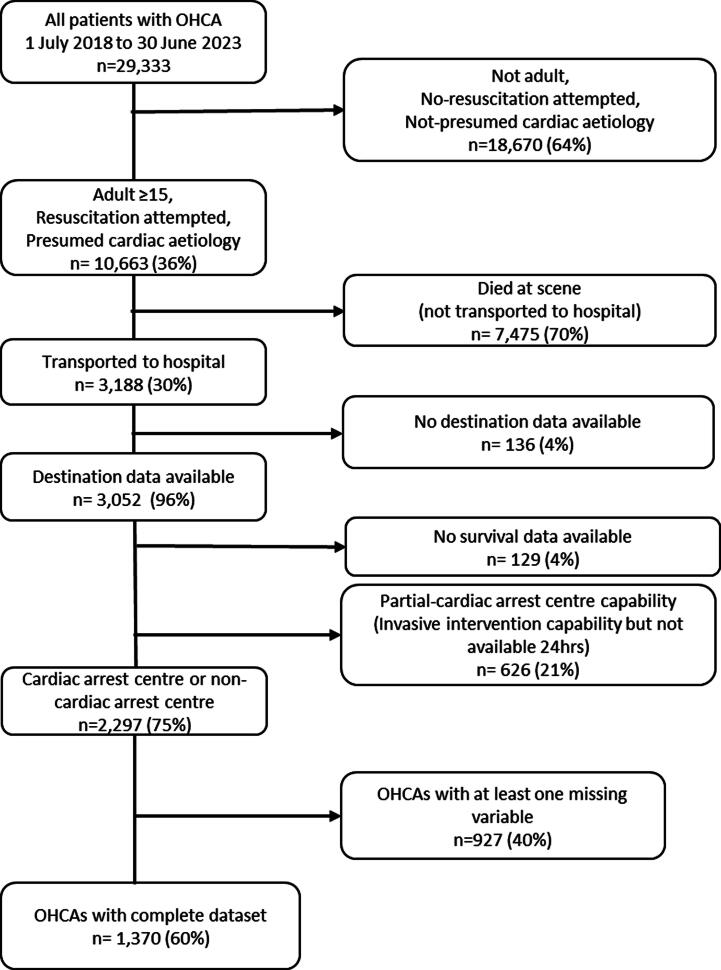
A retrospective cohort study was conducted using the Aotearoa New Zealand Paramedic Care Collection (ANZPaCC) database for adults treated for out-of-hospital cardiac arrest of presumed cardiac aetiology between 1 July 2018 to 30 June 2023. Propensity score-matched analysis was used to investigate survival at 30-days post-event according to the receiving hospital being a cardiac arrest centre versus a non-cardiac arrest centre.
There were 2,297 OHCA patients included. Propensity matching resulted in 554 matched pairs ( = 1108). Thirty-day survival in propensity score-matched patients transported directly to a cardiac arrest centre (56%) versus a non-cardiac arrest centre (45%) was not significantly different (adjusted Odds Ratio 0.78 95%CI 0.54, 1.13, = 0.19). Shockable presenting rhythm, bystander CPR, and presence of STEMI were associated with a higher odds of 30 day survival ( < 0.05). Māori or Pacific Peoples ethnicity and older age were associated with lower survival ( < 0.05).
This study found no statistically significant difference in outcomes for OHCA patients transferred to a cardiac arrest compared to a non-cardiac arrest centre. However, the odds ratio of 0.78, equivalent to a 22% decrease in 30-day mortality, is consistent with benefit associated with management by a cardiac arrest centre. Further research in larger cohorts with detailed information on known outcome predictors, or large randomised clinical trials are needed.
院外心脏骤停后直接转运至心脏骤停中心可能与更高的生存率相关。然而,在新西兰的背景下,支持这一观点的证据有限。本研究采用倾向评分匹配队列来调查在新西兰直接转运至心脏骤停中心是否能提高生存率。
使用新西兰急救护理数据集(ANZPaCC)数据库进行一项回顾性队列研究,研究对象为2018年7月1日至2023年6月30日期间因推测为心脏病因的院外心脏骤停接受治疗的成年人。倾向评分匹配分析用于根据接收医院是心脏骤停中心还是非心脏骤停中心来调查事件发生后30天的生存率。
纳入了2297例院外心脏骤停患者。倾向匹配产生了554对匹配对(n = 1108)。直接转运至心脏骤停中心的倾向评分匹配患者的30天生存率(56%)与转运至非心脏骤停中心的患者(45%)相比,差异无统计学意义(调整后的优势比为0.78,95%置信区间为0.54, 1.13,P = 0.19)。可电击心律、旁观者心肺复苏和ST段抬高型心肌梗死的存在与30天生存几率较高相关(P < 0.05)。毛利族或太平洋岛民族裔以及年龄较大与生存率较低相关(P < 0.05)。
本研究发现,与非心脏骤停中心相比,转至心脏骤停中心的院外心脏骤停患者的结局在统计学上无显著差异。然而,0.78的优势比相当于30天死亡率降低22%,这与心脏骤停中心管理带来的益处一致。需要在更大的队列中进行进一步研究,纳入已知结局预测因素的详细信息,或开展大型随机临床试验。