Roda Domingos, Veiga Pedro, Melo Joana Barbosa, Carreira Isabel Marques, Ribeiro Ilda Patrícia
Algarve Radiation Oncology Unit-Joaquim Chaves Saúde (JCS), 8000-316 Faro, Portugal.
Institute of Cellular and Molecular Biology, Cytogenetics and Genomics Laboratory, Faculty of Medicine, University of Coimbra, 3000-548 Coimbra, Portugal.
Genes (Basel). 2024 Apr 17;15(4):501. doi: 10.3390/genes15040501.
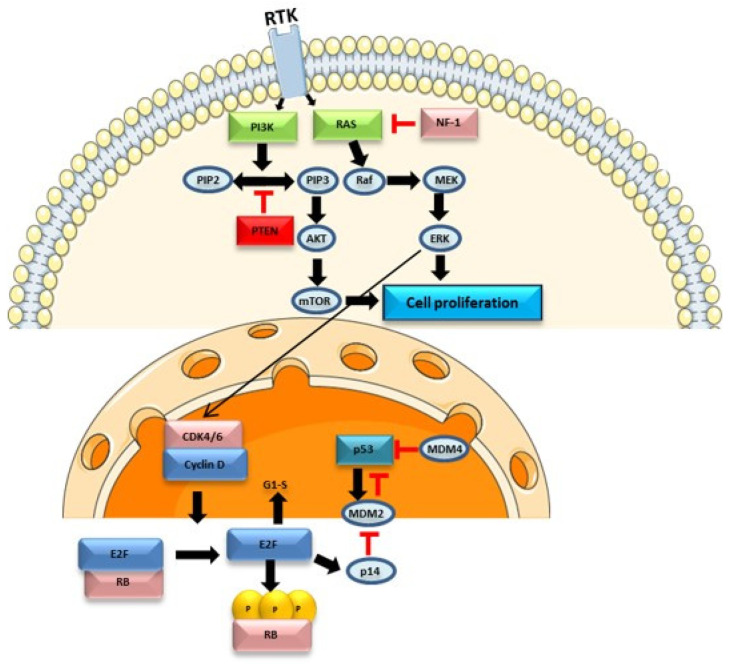
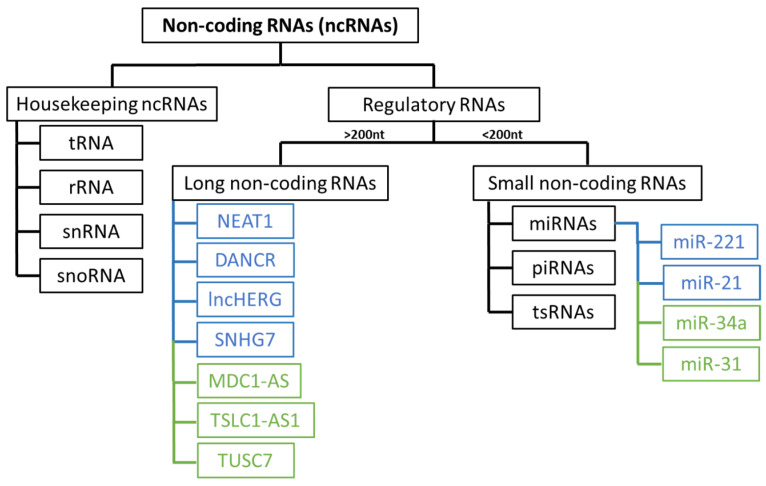
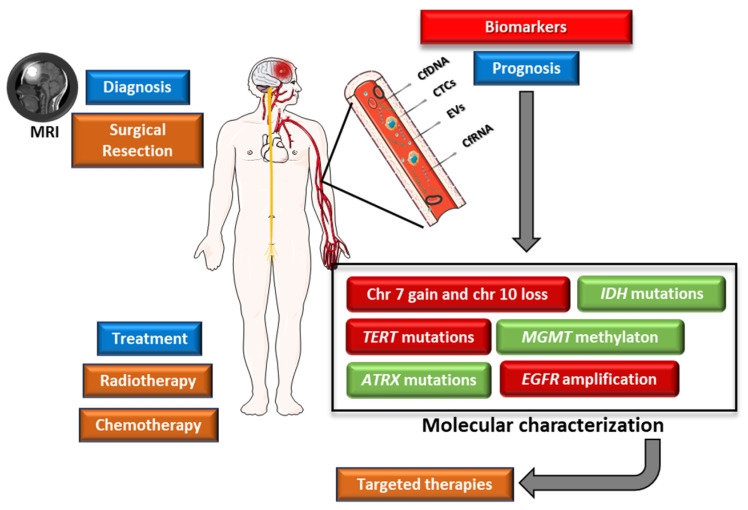
Glioblastoma, the most aggressive and common malignant primary brain tumour, is characterized by infiltrative growth, abundant vascularization, and aggressive clinical evolution. Patients with glioblastoma often face poor prognoses, with a median survival of approximately 15 months. Technological progress and the subsequent improvement in understanding the pathophysiology of these tumours have not translated into significant achievements in therapies or survival outcomes for patients. Progress in molecular profiling has yielded new omics data for a more refined classification of glioblastoma. Several typical genetic and epigenetic alterations in glioblastoma include mutations in genes regulating receptor tyrosine kinase (RTK)/rat sarcoma (RAS)/phosphoinositide 3-kinase (PI3K), p53, and retinoblastoma protein (RB) signalling, as well as mutation of isocitrate dehydrogenase (), methylation of O-methylguanine-DNA methyltransferase (), amplification of epidermal growth factor receptor vIII, and codeletion of 1p/19q. Certain microRNAs, such as miR-10b and miR-21, have also been identified as prognostic biomarkers. Effective treatment options for glioblastoma are limited. Surgery, radiotherapy, and alkylating agent chemotherapy remain the primary pillars of treatment. Only promoter methylation of the gene predicts the benefit from alkylating chemotherapy with temozolomide and it guides the choice of first-line treatment in elderly patients. Several targeted strategies based on tumour-intrinsic dominant signalling pathways and antigenic tumour profiles are under investigation in clinical trials. This review explores the potential genetic and epigenetic biomarkers that could be deployed as analytical tools in the diagnosis and prognostication of glioblastoma. Recent clinical advancements in treating glioblastoma are also discussed, along with the potential of liquid biopsies to advance personalized medicine in the field of glioblastoma, highlighting the challenges and promises for the future.
胶质母细胞瘤是最具侵袭性且常见的原发性恶性脑肿瘤,其特征为浸润性生长、丰富的血管生成以及侵袭性的临床进展。胶质母细胞瘤患者的预后通常较差,中位生存期约为15个月。技术进步以及随后对这些肿瘤病理生理学理解的改善并未转化为患者治疗或生存结果的显著成就。分子谱分析的进展产生了新的组学数据,用于对胶质母细胞瘤进行更精细的分类。胶质母细胞瘤中几种典型的基因和表观遗传改变包括调节受体酪氨酸激酶(RTK)/大鼠肉瘤(RAS)/磷酸肌醇3激酶(PI3K)、p53和视网膜母细胞瘤蛋白(RB)信号通路的基因突变,以及异柠檬酸脱氢酶()突变、O -甲基鸟嘌呤 - DNA甲基转移酶()甲基化、表皮生长因子受体vIII扩增和1p/19q共缺失。某些微小RNA,如miR - 10b和miR - 21,也已被确定为预后生物标志物。胶质母细胞瘤的有效治疗选择有限。手术、放疗和烷基化剂化疗仍然是主要的治疗支柱。只有基因的启动子甲基化可预测替莫唑胺烷基化化疗的获益情况,并指导老年患者一线治疗的选择。基于肿瘤内在主导信号通路和抗原性肿瘤谱的几种靶向策略正在临床试验中进行研究。本综述探讨了可能作为分析工具用于胶质母细胞瘤诊断和预后的潜在遗传和表观遗传生物标志物。还讨论了胶质母细胞瘤治疗的最新临床进展,以及液体活检在胶质母细胞瘤领域推进个性化医疗的潜力,强调了未来的挑战和前景。