Wozniak Hannah, Tabah Alexis, Barbier François, Ruckly Stéphane, Loiodice Ambre, Akova Murat, Leone Marc, Conway Morris Andrew, Bassetti Matteo, Arvaniti Kostoula, Ferrer Ricard, de Bus Liesbet, Paiva Jose Artur, Bracht Hendrik, Mikstacki Adam, Alsisi Adel, Valeanu Liana, Prazak Josef, Timsit Jean-François, Buetti Niccolò
Division of Critical Care, Department of Acute Medicine, University Hospital of Geneva, University of Geneva, Geneva, Switzerland.
Interdepartmental Division of Critical Care Medicine, University of Toronto, Toronto, Canada.
Ann Intensive Care. 2024 May 2;14(1):70. doi: 10.1186/s13613-024-01299-x.
Hospital-acquired bloodstream infections are common in the intensive care unit (ICU) and have a high mortality rate. Patients with cirrhosis are especially susceptible to infections, yet there is a knowledge gap in the epidemiological distinctions in hospital-acquired bloodstream infections between cirrhotic and non-cirrhotic patients in the ICU. It has been suggested that cirrhotic patients, present a trend towards more gram-positive infections, and especially enterococcal infections. This study aims to describe epidemiological differences in hospital-acquired bloodstream infections between cirrhotic and non-cirrhotic patients hospitalized in the ICU regarding infection sources, microorganisms and mortality.
Using prospective Eurobact-2 international cohort study data, we compared hospital-acquired bloodstream infections sources and microorganisms in cirrhotic and non-cirrhotic patients. The association between Enterococcus faecium and cirrhosis was studied using a multivariable mixed logistic regression. The association between cirrhosis and mortality was assessed by a multivariable frailty Cox model.
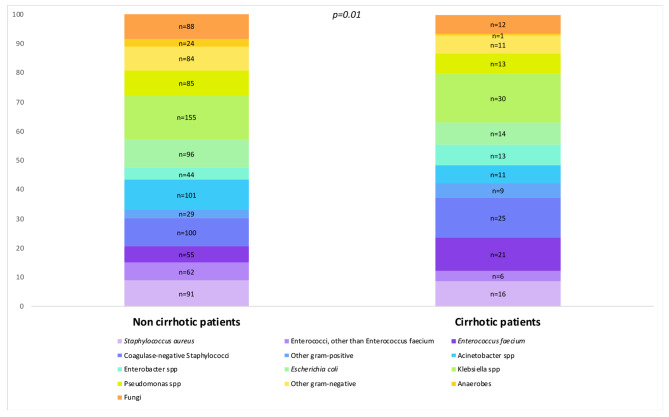
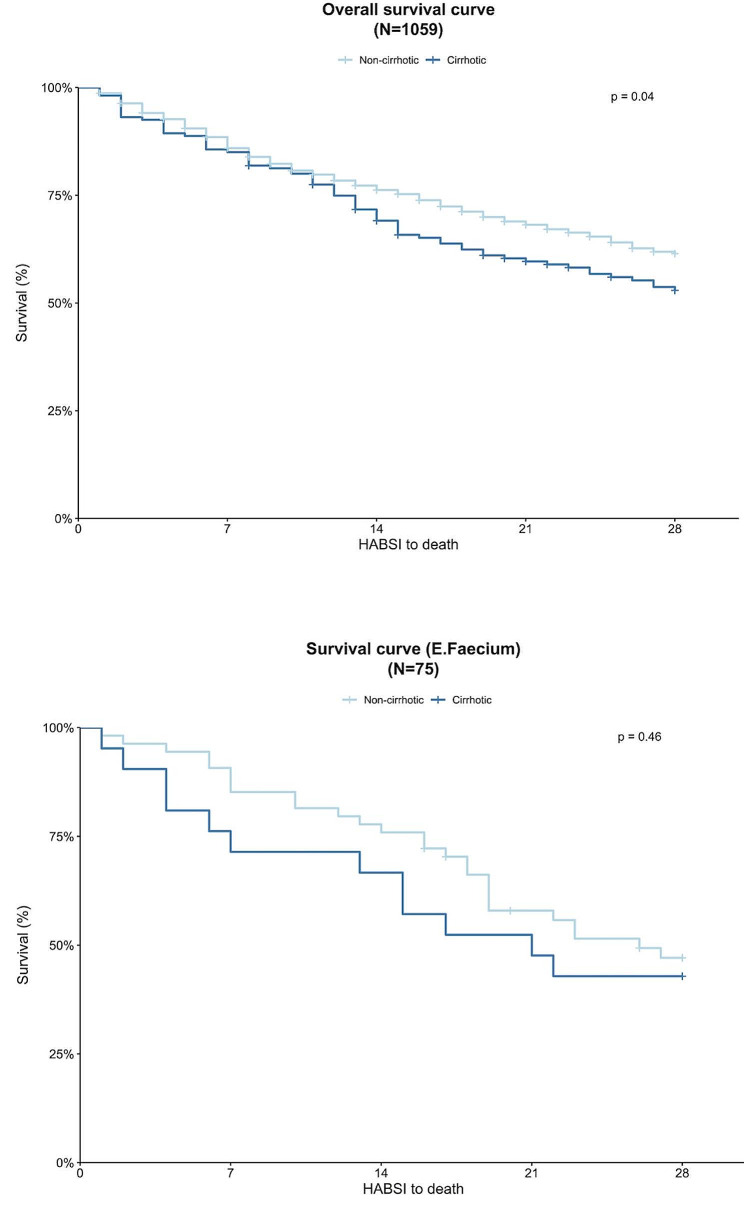
Among the 1059 hospital-acquired bloodstream infections patients included from 101 centers, 160 had cirrhosis. Hospital-acquired bloodstream infection source in cirrhotic patients was primarily abdominal (35.6%), while it was pulmonary (18.9%) for non-cirrhotic (p < 0.01). Gram-positive hospital-acquired bloodstream infections accounted for 42.3% in cirrhotic patients compared to 33.2% in non-cirrhotic patients (p = 0.02). Hospital-acquired bloodstream infections in cirrhotic patients were most frequently caused by Klebsiella spp (16.5%), coagulase-negative Staphylococci (13.7%) and E. faecium (11.5%). E. faecium bacteremia was more frequent in cirrhotic patients (11.5% versus 4.5%, p < 0.01). After adjusting for possible confounding factors, cirrhosis was associated with higher E. faecium hospital-acquired bloodstream infections risk (Odds ratio 2.5, 95% CI 1.3-4.5, p < 0.01). Cirrhotic patients had increased mortality compared to non-cirrhotic patients (Hazard Ratio 1.3, 95% CI 1.01-1.7, p = 0.045).
Critically ill cirrhotic patients with hospital-acquired bloodstream infections exhibit distinct epidemiology, with more Gram-positive infections and particularly Enterococcus faecium.
医院获得性血流感染在重症监护病房(ICU)很常见,且死亡率很高。肝硬化患者尤其易受感染,但在ICU中,肝硬化患者与非肝硬化患者医院获得性血流感染的流行病学差异方面存在知识空白。有人提出,肝硬化患者有革兰氏阳性菌感染增加的趋势,尤其是肠球菌感染。本研究旨在描述ICU中住院的肝硬化患者与非肝硬化患者在医院获得性血流感染方面在感染源、微生物和死亡率上的流行病学差异。
利用前瞻性欧洲细菌-2国际队列研究数据,我们比较了肝硬化患者与非肝硬化患者医院获得性血流感染的来源和微生物。使用多变量混合逻辑回归研究粪肠球菌与肝硬化之间的关联。通过多变量脆弱性Cox模型评估肝硬化与死亡率之间的关联。
在来自101个中心的1059例医院获得性血流感染患者中,160例患有肝硬化。肝硬化患者医院获得性血流感染的来源主要是腹部(35.6%),而非肝硬化患者为肺部(18.9%)(p<0.01)。肝硬化患者革兰氏阳性菌医院获得性血流感染占42.3%,而非肝硬化患者为33.2%(p=0.02)。肝硬化患者医院获得性血流感染最常见的致病菌为克雷伯菌属(16.5%)、凝固酶阴性葡萄球菌(13.7%)和粪肠球菌(11.5%)。粪肠球菌血症在肝硬化患者中更常见(11.5%对4.5%,p<0.01)。在调整可能的混杂因素后,肝硬化与粪肠球菌医院获得性血流感染风险较高相关(比值比2.5,95%置信区间1.3-4.5,p<0.01)。与非肝硬化患者相比,肝硬化患者死亡率增加(风险比1.3,95%置信区间1.01-1.7,p=0.045)。
患有医院获得性血流感染的重症肝硬化患者表现出独特的流行病学特征——革兰氏阳性菌感染更多,尤其是粪肠球菌感染。