Department for Developmental Origins of Disease, University Medical Center Utrecht Brain Center and Wilhelmina Children's Hospital, Utrecht University, Internal post: KC03.068.0, PO Box 85090, Utrecht, 3508 AB, The Netherlands.
Anatomy & Neurosciences, Amsterdam UMC, location Vrije Universiteit Amsterdam, De Boelelaan 1117, Amsterdam, The Netherlands.
Stem Cell Res Ther. 2024 May 7;15(1):134. doi: 10.1186/s13287-024-03747-8.
Hypoxic-Ischemic Encephalopathy (HIE) is a leading cause of mortality and morbidity in newborns. Recent research has shown promise in using intranasal mesenchymal stem cell (MSC) therapy if administered within 10 days after Hypoxia-Ischemia (HI) in neonatal mice. MSCs migrate from the nasal cavity to the cerebral lesion in response to chemotactic cues. Which exact chemokines are crucial for MSC guidance to the HI lesion is currently not fully understood. This study investigates the role of CXCL10 in MSC migration towards the HI-injured brain.
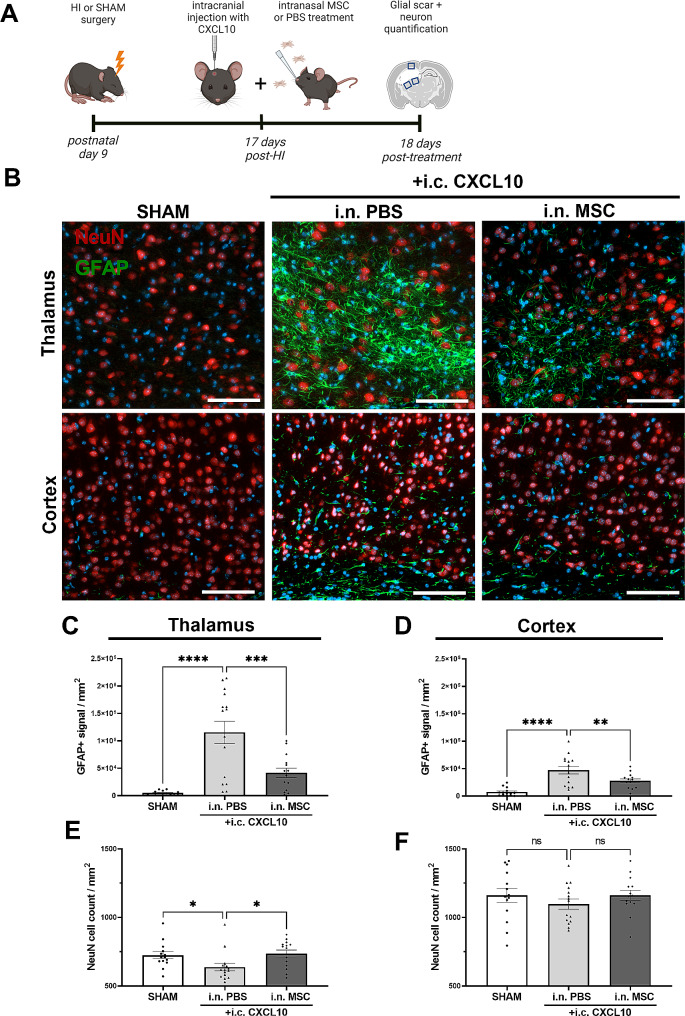
HI was induced in male and female 9-day-old C57BL/6 mice followed by intranasal MSC treatment at day 10 or 17 post-HI. CXCL10 protein levels, PKH26-labeled MSCs and lesion size were assessed by ELISA, immunofluorescent imaging and MAP2 staining respectively. At day 17 post-HI, when CXCL10 levels were reduced, intracranial CXCL10 injection and intranasal PKH26-labeled MSC administration were combined to assess CXCL10-guided MSC migration. MSC treatment efficacy was evaluated after 18 days, measuring lesion size, motor outcome (cylinder rearing task), glial scarring (GFAP staining) and neuronal density (NeuN staining) around the lesion. Expression of the receptor for CXCL10, i.e. CXCR3, on MSCs was confirmed by qPCR and Western Blot. Moreover, CXCL10-guided MSC migration was assessed through an in vitro transwell migration assay.
Intranasal MSC treatment at day 17 post-HI did not reduce lesion size in contrast to earlier treatment timepoints. Cerebral CXCL10 levels were significantly decreased at 17 days versus 10 days post-HI and correlated with reduced MSC migration towards the brain. In vitro experiments demonstrated that CXCR3 receptor inhibition prevented CXCL10-guided migration of MSCs. Intracranial CXCL10 injection at day 17 post-HI significantly increased the number of MSCs reaching the lesion which was accompanied by repair of the HI lesion as measured by reduced lesion size and glial scarring, and an increased number of neurons around the lesion.
This study underscores the crucial role of the chemoattractant CXCL10 in guiding MSCs to the HI lesion after intranasal administration. Strategies to enhance CXCR3-mediated migration of MSCs may improve the efficacy of MSC therapy or extend its regenerative therapeutic window.
缺氧缺血性脑病(HIE)是新生儿死亡和发病的主要原因。最近的研究表明,在新生小鼠缺氧缺血(HI)后 10 天内使用鼻内间充质干细胞(MSC)治疗具有潜力。MSC 从鼻腔迁移到大脑病变部位,以响应趋化因子的趋化作用。目前尚不完全清楚哪些确切的趋化因子对 MSC 向 HI 病变的引导至关重要。本研究旨在探讨 CXCL10 在 MSC 向 HI 损伤大脑迁移中的作用。
在雄性和雌性 9 天大的 C57BL/6 小鼠中诱导 HI,然后在 HI 后第 10 天或第 17 天进行鼻内 MSC 治疗。通过 ELISA、免疫荧光成像和 MAP2 染色分别评估 CXCL10 蛋白水平、PKH26 标记的 MSC 和病变大小。在 HI 后第 17 天,当 CXCL10 水平降低时,将颅内 CXCL10 注射和鼻内 PKH26 标记的 MSC 给药相结合,以评估 CXCL10 引导的 MSC 迁移。在 HI 后第 18 天,通过测量病变大小、运动结果(圆筒饲养任务)、神经胶质瘢痕(GFAP 染色)和病变周围神经元密度(NeuN 染色)来评估 MSC 治疗效果。通过 qPCR 和 Western Blot 证实 MSC 上 CXCL10 受体即 CXCR3 的表达。此外,通过体外 Transwell 迁移实验评估 CXCL10 引导的 MSC 迁移。
与较早的治疗时间点相比,HI 后第 17 天进行鼻内 MSC 治疗并未减少病变大小。与 HI 后第 10 天相比,第 17 天大脑中的 CXCL10 水平显著降低,与 MSC 向大脑的迁移减少相关。体外实验表明,CXCR3 受体抑制可阻止 CXCL10 引导的 MSC 迁移。在 HI 后第 17 天颅内注射 CXCL10 可显著增加到达病变部位的 MSC 数量,这伴随着 HI 病变的修复,表现为病变体积缩小和神经胶质瘢痕减少,以及病变周围神经元数量增加。
本研究强调了趋化因子 CXCL10 在鼻内给药后引导 MSC 到达 HI 病变部位的关键作用。增强 MSC 与 CXCR3 介导的迁移的策略可能会提高 MSC 治疗的疗效或延长其再生治疗窗口。