Department of Rehabilitation Medicine, First Hospital of Jilin University, Changchun, China.
J Neuroeng Rehabil. 2024 May 14;21(1):77. doi: 10.1186/s12984-024-01372-3.
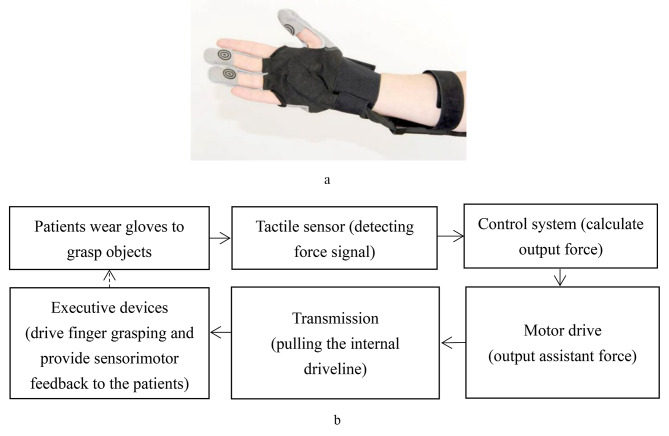
Over 80% of patients with stroke experience finger grasping dysfunction, affecting independence in activities of daily living and quality of life. In routine training, task-oriented training is usually used for functional hand training, which may improve finger grasping performance after stroke, while augmented therapy may lead to a better treatment outcome. As a new technology-supported training, the hand rehabilitation robot provides opportunities to improve the therapeutic effect by increasing the training intensity. However, most hand rehabilitation robots commonly applied in clinics are based on a passive training mode and lack the sensory feedback function of fingers, which is not conducive to patients completing more accurate grasping movements. A force feedback hand rehabilitation robot can compensate for these defects. However, its clinical efficacy in patients with stroke remains unknown. This study aimed to investigate the effectiveness and added value of a force feedback hand rehabilitation robot combined with task-oriented training in stroke patients with hemiplegia.
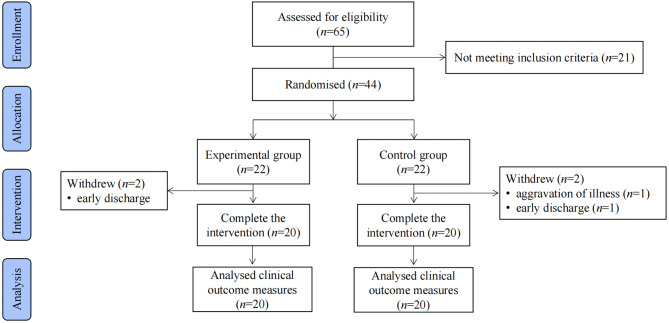
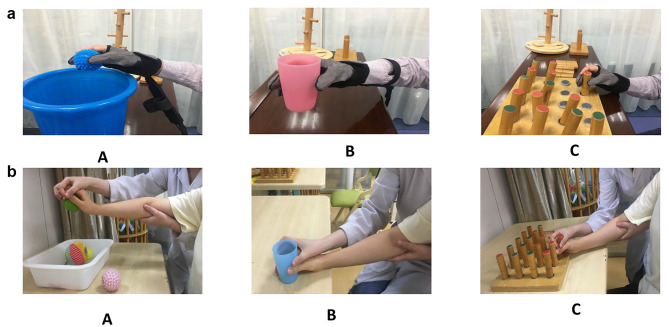
In this single-blinded randomised controlled trial, 44 stroke patients with hemiplegia were randomly divided into experimental (n = 22) and control (n = 22) groups. Both groups received 40 min/day of conventional upper limb rehabilitation training. The experimental group received 20 min/day of task-oriented training assisted by a force feedback rehabilitation robot, and the control group received 20 min/day of task-oriented training assisted by therapists. Training was provided for 4 weeks, 5 times/week. The Fugl-Meyer motor function assessment of the hand part (FMA-Hand), Action Research Arm Test (ARAT), grip strength, Modified Ashworth scale (MAS), range of motion (ROM), Brunnstrom recovery stages of the hand (BRS-H), and Barthel index (BI) were used to evaluate the effect of two groups before and after treatment.
Intra-group comparison: In both groups, the FMA-Hand, ARAT, grip strength, AROM, BRS-H, and BI scores after 4 weeks of treatment were significantly higher than those before treatment (p < 0.05), whereas there was no significant difference in finger flexor MAS scores before and after treatment (p > 0.05). Inter-group comparison: After 4 weeks of treatment, the experimental group's FMA-Hand total score, ARAT, grip strength, and AROM were significantly better than those of the control group (p < 0.05). However, there were no statistically significant differences in the scores of each sub-item of the FMA-Hand after Bonferroni correction (p > 0.007). In addition, there were no statistically significant differences in MAS, BRS-H, and BI scores (p > 0.05).
Hand performance improved in patients with stroke after 4 weeks of task-oriented training. The use of a force feedback hand rehabilitation robot to support task-oriented training showed additional value over conventional task-oriented training in stroke patients with hand dysfunction.
NCT05841108.
超过 80%的中风患者存在手指抓握功能障碍,这会影响日常生活活动和生活质量的独立性。在常规训练中,通常使用任务导向训练进行手部功能训练,这可能会改善中风后的手指抓握能力,而增强疗法可能会带来更好的治疗效果。作为一种新的技术支持的训练,手部康复机器人通过增加训练强度为提高治疗效果提供了机会。然而,临床上常用的大多数手部康复机器人都基于被动训练模式,缺乏手指的感觉反馈功能,不利于患者完成更精确的抓握动作。力反馈手部康复机器人可以弥补这些缺陷。然而,其在中风患者中的临床疗效尚不清楚。本研究旨在探讨力反馈手部康复机器人结合任务导向训练在偏瘫中风患者中的有效性和附加价值。
这是一项单盲随机对照试验,纳入 44 名偏瘫中风患者,随机分为实验组(n=22)和对照组(n=22)。两组均接受 40 分钟/天的常规上肢康复训练。实验组接受 20 分钟/天的任务导向训练,由力反馈康复机器人辅助,对照组接受 20 分钟/天的任务导向训练,由治疗师辅助。治疗持续 4 周,每周 5 次。采用 Fugl-Meyer 上肢运动功能评估(FMA-Hand)、上肢动作研究测试(ARAT)、握力、改良 Ashworth 量表(MAS)、关节活动度(ROM)、手部 Brunnstrom 恢复阶段(BRS-H)和 Barthel 指数(BI)评估两组治疗前后的效果。
组内比较:两组治疗 4 周后 FMA-Hand 总分、ARAT、握力、主动ROM、BRS-H 和 BI 评分均明显高于治疗前(p<0.05),而手指屈肌 MAS 评分治疗前后无明显差异(p>0.05)。组间比较:治疗 4 周后,实验组 FMA-Hand 总分、ARAT、握力和主动 ROM 明显优于对照组(p<0.05)。然而,经 Bonferroni 校正后,FMA-Hand 各亚项评分无统计学差异(p>0.007)。此外,MAS、BRS-H 和 BI 评分无统计学差异(p>0.05)。
任务导向训练 4 周后,中风患者手部功能得到改善。使用力反馈手部康复机器人支持任务导向训练,与常规任务导向训练相比,对中风后手部功能障碍患者具有附加价值。
NCT05841108。