University of Sousse, Farhat Hached hospital. Laboratory of physiology and functional explorations, Sousse, Tunisia.
University of Sousse, Farhat Hached hospital. Heart failure (LR12SP09) research laboratory, Sousse, Tunisia.
Tunis Med. 2024 May 5;102(5):266-271. doi: 10.62438/tunismed.v102i5.4871.
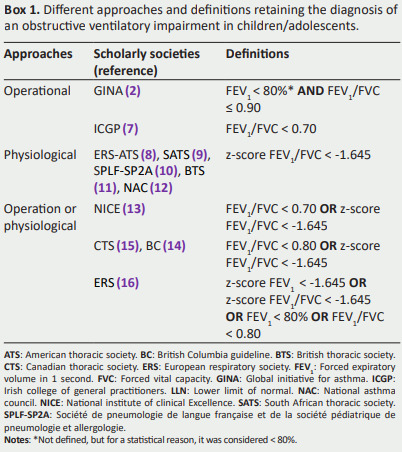
There is no clear consensus as to what constitutes an obstructive ventilatory impairment (OVI) in pediatric populations.
To determine the percentage of children/adolescents having an OVI among those addressed for spirometry after taking into account the definitions advanced by some international scholarly societies [British Columbia (BC), British thoracic-society (BTS), Canadian thoracic society (CTS), European respiratory society and American thoracic society (ERS-ATS), global initiative for asthma (GINA), Irish college of general practitioners (ICGP), national asthma council (NAC), national institute of clinical excellence (NICE), Société de pneumologie de langue française, Société pédiatrique de pneumologie et allergologie (SPLF-SP2A), and South African thoracic society (SATS)].
This bi-centric cross-sectional study involves two medical structures in Sousse/Tunisia, and will encompass children/adolescents aged 6-18 years. A medical questionnaire will be administered, clinical and anthropometric data will be collected, and the spirometric data will be measured by two spirometers. The following six definitions of OVI will be applied: i) GINA: Forced expiratory volume in 1 second (FEV1) < 80% and a FEV1/forced vital capacity (FVC) ≤ 0.90; ii) ICGP: FEV1/FVC < 0.70; iii) ERS-ATS or BTS or SATS or SPLF-SP2A or NAC: FEV1/FVC z-score < -1.645; iv) NICE: FEV1/FVC < 0.70 or FEV1/FVC z-score < -1.645; v) CTS: FEV1/FVC < 0.80 or a FEV1/FVC z-score < -1.645; and vi) ERS: "FEV1 z-score or FEV1/FVC z-score" < -1.645 or "FEV1 or FEV1/FVC" < 0.80.
The percentage of children/adolescents having an OVI will significantly vary between the six definitions.
The frequency of OVI in a pediatric population will depend on the definition chosen.
目前,对于儿科人群中的阻塞性通气功能障碍(OVI)的定义尚未达成明确共识。
通过考虑一些国际学术协会(不列颠哥伦比亚省(BC)、英国胸科学会(BTS)、加拿大胸科学会(CTS)、欧洲呼吸学会和美国胸科学会(ERS-ATS)、全球哮喘倡议(GINA)、爱尔兰普通医生学院(ICGP)、国家哮喘理事会(NAC)、国家临床卓越研究所(NICE)、法国呼吸学会、儿科呼吸病学和过敏学会(SPLF-SP2A)以及南非胸科学会(SATS))提出的定义,来确定在接受肺量计检查的儿童/青少年中,OVI 的比例。
这是一项涉及突尼斯苏塞的两个医疗结构的双中心横断面研究,将包括 6-18 岁的儿童/青少年。将进行一份医学问卷,收集临床和人体测量数据,并使用两台肺量计测量肺量计数据。将应用以下六种 OVI 定义:i)GINA:第 1 秒用力呼气量(FEV1)<80%且 FEV1/用力肺活量(FVC)≤0.90;ii)ICGP:FEV1/FVC<0.70;iii)ERS-ATS 或 BTS 或 SATS 或 SPLF-SP2A 或 NAC:FEV1/FVC z 评分<-1.645;iv)NICE:FEV1/FVC<0.70 或 FEV1/FVC z 评分<-1.645;v)CTS:FEV1/FVC<0.80 或 FEV1/FVC z 评分<-1.645;和 vi)ERS:“FEV1 z 评分或 FEV1/FVC z 评分”<-1.645 或“FEV1 或 FEV1/FVC”<0.80。
在这六种定义中,儿童/青少年 OVI 的比例将有显著差异。
儿科人群中 OVI 的频率将取决于所选的定义。